
CDHO Advisory: Hypertension
COLLEGE OF DENTAL HYGIENISTS OF ONTARIO ADVISORY
ADVISORY TITLE
Use of the dental hygiene interventions of scaling of teeth and root planing including curetting surrounding tissue, orthodontic and restorative practices, and other invasive interventions for persons1 with hypertension.
ADVISORY STATUS
Cite as College of Dental Hygienists of Ontario, CDHO Advisory Hypertension, 2023-04-18
INTERVENTIONS AND PRACTICES CONSIDERED
Scaling of teeth and root planing including curetting surrounding tissue, orthodontic and restorative practices, and other invasive interventions (“the Procedures”).
SCOPE
DISEASE/CONDITION(S)/PROCEDURE(S)
Hypertension
INTENDED USERS
Advanced practice nurses
Dental assistants
Dental hygienists
Dentists
Denturists
Dieticians
Health professional students
Nurses
Patients/clients
Pharmacists
Physicians
Public health departments
Regulatory bodies
ADVISORY OBJECTIVE(S)
To guide dental hygienists at the point of care relative to the use of the Procedures for persons who have hypertension, chiefly as follows.
- Understanding the medical condition.
- Sourcing medications information.
- Taking the medical and medications history.
- Identifying and contacting the most appropriate healthcare provider(s) for medical advice.
- Understanding and taking appropriate precautions prior to and during the Procedures proposed.
- Deciding when and when not to proceed with the Procedures proposed.
- Dealing with adverse events arising during the Procedures.
- Keeping records.
- Advising the patient/client.
TARGET POPULATION
Child (2 to 12 years)
Adolescent (13 to 18 years)
Adult (19 to 44 years)
Middle Age (45 to 64 years)
Aged (65 to 79 years)
Aged 80 and over
Male
Female
Parents, guardians, and family caregivers of children, young persons and adults with hypertension.
MAJOR OUTCOMES CONSIDERED
For persons who have hypertension: to maximize health benefits and minimize adverse effects by promoting the performance of the Procedures at the right time with the appropriate precautions, and by discouraging the performance of the Procedures at the wrong time or in the absence of appropriate precautions.
RECOMMENDATIONS
UNDERSTANDING THE MEDICAL CONDITION
Terminology used in this Advisory
Resources consulted
- High blood pressure, hypertensive crisis (hypertension): Mayo Clinic
- Hypertension: Hypertension Canada
- Hypertension: MedlinePlus
Hypertension
- refers to blood pressure that persistently exceeds specified limits in adults or specified percentiles for sex, age, and height in children/adolescents
- is sometimes classified by
- the absence or presence of identifiable cause, as in
- essential hypertension, lacks identifiable cause, represents 90 percent of diagnoses of hypertension
- secondary hypertension, linked to one or more identifiable causes, such as medical conditions or medications, including
- aldosteronism (CDHO Advisory) in which an adrenal gland tumour causes excessive release of the hormone aldosterone, which raises blood pressure because the kidneys
- retain salt and water
- lose too much potassium
- coarctation of the aorta, congenital narrowing of the aorta, which causes the heart to pump with increased force, which
- is necessary to get blood through the aorta
- raises the blood pressure
- Cushing’s syndrome (CDHO Advisory) in which a pituitary tumour or other abnormalities cause the adrenal glands to produce too much cortisol, which increases the blood pressure
- diabetes (CDHO Advisory) complications of which cause kidney damage leading to high blood pressure
- glomerular disease, a type of kidney disease (CDHO Advisory) in which problems with the kidney’s filters lead to high blood pressure
- hyperparathyroidism, excessive secretion of parathyroid hormone which increases blood calcium and leads to increased blood pressure
- hyperthyroidism (CDHO Advisory), excessive secretion of thyroid hormone leading to high blood pressure
- hypothyroidism (CDHO Advisory), insufficient secretion of thyroid hormone leading to high blood pressure
- medications, supplements may raise blood pressure
- substances of abuse (CDHO Advisory) may increase blood pressure
- obesity (CDHO Advisory) raises blood pressure by
- putting pressure on artery walls
- increasing heart rate
- pheochromocytoma, rare adrenal gland tumour, increases production of adrenaline and noradrenaline, which raises blood pressure
- polycystic kidney disease (CDHO Advisory), in which kidney cysts impair kidney function and may lead to raised blood pressure
- pregnancy (CDHO Advisory) may
- exacerbate existing high blood pressure
- cause high blood pressure leading to a potentially dangerous condition, preeclampsia, also termed pregnancy-induced hypertension
- renovascular hypertension
- sleep apnea (CDHO Advisory), often marked by severe snoring, in which breathing repeatedly stops and starts during sleep, causing oxygen deprivation which, through a sequence of effects, increases blood pressure
- aldosteronism (CDHO Advisory) in which an adrenal gland tumour causes excessive release of the hormone aldosterone, which raises blood pressure because the kidneys
- specific parts of the vascular system in which it occurs, such as
- portal hypertension, in which impairment of blood flow in the liver causes varicosities of the portal vein; commonly associated with cirrhosis of the liver
- pulmonary hypertension, a rare disorder of the blood vessels of the lung in which the pressure in the pulmonary artery increases even to the point of becoming life-threatening; sometimes the cause is identifiable, sometimes not
- renovascular hypertension, narrowing of the arteries that carry blood to the kidneys, most commonly associated with atherosclerosis of these arteries
- severity, medical condition or health status, such as
- malignant hypertension, very high blood pressure which
- develops suddenly
- is a severe and dangerous form of high blood pressure
- is associated with papilledema
- is an emergency condition which can be life-threatening
- vascular disorders, such as heart disease, which may be consequences as well as causes of hypertension
- kidney disorders, may be consequences as well as causes of hypertension
- preeclampsia, hypertension and proteinuria that develops after week 20 of pregnancy
- endocrine hypertension, overproduction of aldosterone by the adrenal gland caused by malfunction or tumour, which leads to fluid retention and increased blood pressure.
- malignant hypertension, very high blood pressure which
- the absence or presence of identifiable cause, as in
Other terminology
- Abdominal aortic aneurysm, when the aorta becomes abnormally large or balloons outward, creating the risk of rupture, a major medical emergency.
- Atherosclerosis, disease of large and medium-sized arteries in muscles, which
- is characterized by hardening and narrowing of the arteries caused by the accumulation of fatty deposits called plaque
- may cause a blood clot to form at the site of the narrowing, which completely
- blocks the artery
- and, in a coronary artery, causes myocardial infarction (CDHO Advisory).
- Body Mass Index (BMI) body weight in kg divided by height in metres squared (kg/m2).
- Cardiac dysrhythmia, cardiac arrhythmia, irregular or abnormal heart rate.
- Dyspnea, shortness of breath, breathlessness.
- Hypertensive crisis, a severe increase in blood pressure that creates
- urgency, where blood pressures is dangerously high but has not apparently caused damage to any organ
- emergency, where blood pressure is dangerously high and
- has caused damage to an organ
- may be associated with life-threatening complications, such as a stroke.
- Hypertensive retinopathy, damage to the blood vessels in the retina caused by high blood pressure, which may result in serious effects on vision.
- Lichen planus, a chronic mucocutaneous disease affecting the skin, nails, and/or any lining mucosa (including in the mouth).
- Papilledema, swelling of the optic nerve behind the eye.
- Peripheral arterial disease, narrowing and hardening of the arteries that supply the legs and feet, caused by arteriosclerosis.
Overview of hypertension
Resources consulted
- College of Dental Hygienists of Ontario: Hypertension in Adults Fact Sheet
- College of Dental Hygienists of Ontario: Hypertension in Children & Adolescents Fact Sheet
- Diagnosing Secondary Hypertension: American Academy of Family Physicians
- Getting your blood pressure in check: Heart and Stroke Foundation
- Hypertension in children: Journal of Dental Education
- Hypertension: Medline Plus
- Mortality among patients with hypertension from 1995 to 2005: a population-based study | Canadian Medical Association Journal
- Hypertension: Hypertension Canada (including Hypertension in Canada Fact Sheet: May 2016)
Occurrence of hypertension
Hypertension
- affects more than one in five Canadian adults, as well as 1 percent to 2 percent of Canadian children/ adolescents (with higher rates amongst those who are overweight or have obesity)
- is frequently asymptomatic: 43 percent of adult Canadians are unaware that they have high blood pressure, though a single high reading may not indicate hypertension
- increases in frequency with age: about half of persons aged 65 to 74 have hypertension
- appears to be more common in developed rather than developing countries
- occurs as pulmonary hypertension in children, though rarely, as well as adults, as a condition which
- is thought to be genetically determined in up to 10 percent of cases
- occurs in children with congenital heart disease
- is usually detected during well-child examinations because in mild form it is asymptomatic
- may be associated with
- cardiovascular disease
- cystic fibrosis
- family history of cardiovascular disease
- kidney disease
- lung infection
- obesity
- occurs as renovascular hypertension, associated with severe and difficult-to-control hypertension.
Cause of hypertension
Hypertension
- in 90 percent of instances (and in a majority of children/adolescents, particularly in those who are older) is essential hypertension which, by definition, lacks identifiable cause
- in 10 percent of instances (and in a minority of children/adolescents, particularly those who are younger) is secondary hypertension, which has various identifiable causes.
Risk factors of hypertension
- for development of hypertension, include
- absence of symptoms, a common phenomenon, which leads to the development of heart disease and kidney problems without the person’s awareness of high blood pressure
- lifestyle, which accounts for 60 percent of cases, and includes
- abdominal obesity
- excessive alcohol consumption
- physical inactivity
- smoking or exposure to cigarette smoke
- stress
- unhealthy diet, including excessive use of salt (sodium chloride)
- genetic predisposition, which accounts for 35 percent of cases
- Black, Aboriginal, or South Asian ethnicity
- family history of high blood pressure
- underlying disease, such as
- diabetes
- kidney disease
- severe periodontal disease, which may be a risk factor for cardiovascular disease and hypertension
- excessive use of certain medications, such as non-steroidal anti-inflammatory drugs (NSAIDs), which accounts for 5 percent of cases
- arising from hypertension
- when blood pressure is not well controlled include
- abdominal aortic aneurysm
- dementia (CDHO Advisory)
- heart attack (CDHO Advisory)
- heart failure (CDHO Advisory)
- hypertensive retinopathy
- kidney disease, kidney failure (CDHO Advisory)
- peripheral arterial disease
- premature death, which is the
- leading risk for premature death in women
- second leading risk for premature death in men in countries like Canada
- erectile dysfunction
- stroke (CDHO Advisory)
- involve comorbidities, complications and associated conditions
- when blood pressure is not well controlled include
Signs and symptoms of hypertension
Hypertension
- that has created hypertensive crisis is signalled by signs and symptoms that variously include
- anxiety, severe
- chest pain, severe
- dyspnea
- headache, severe and accompanied by confusion and blurred vision
- nausea and vomiting
- seizures (CDHO Advisory)
- unresponsiveness
- is frequently asymptomatic so that, in most instances, high blood pressure is found during routine health checks that include blood pressure measurement
- when symptomatic, may be manifested by the symptoms of
- malignant hypertension, variously
- severe headache
- nausea or vomiting
- confusion
- visual changes
- nosebleeds
- hypertension’s comorbidities, complications and associated conditions
- malignant hypertension, variously
Medical investigation of hypertension
Hypertension is diagnosed according to criteria that require
- assessment of the medical history, medications history, comorbidities, complications and associated conditions
- accurate measurements of systolic and diastolic blood pressure, which
- trigger recommendations for follow up
- take account of variations that depend on the
- time of day
- circumstances, such as a clinical office or home
- when taken at home with an approved device used correctly may be more accurate than blood pressure readings taken in a clinical office
- tests
- of blood cholesterol levels
- for heart disease, such as echocardiogram or electrocardiogram
- for kidney disease, such as lab tests
- to assess metabolism, over which the kidneys exercise considerable influence
- to assess kidney function.
Treatment of hypertension
Hypertension is aimed at
- urgent or emergency response to hypertensive crisis
- emergency response to malignant hypertension
- reduction of blood pressure to lower the risk of complications
- the person’s meeting a target blood pressure
- lifestyle changes in the early stages of hypertension, such as those used in prevention
- medication in the later stages of hypertension or when lifestyle changes prove insufficient.
Prevention of hypertension
Hypertension
- should be monitored for and brought under control by
- use of all appropriate healthcare visits to assess blood pressure by health care professionals specifically trained to measure blood pressure accurately
- by regular checking of blood pressure for patients/clients starting at age 3 years (including those considered at particular risk of hypertension aged 3+ to 5 years)2, and especially for adults
- use of approved devices and proper techniques to measure blood pressure at home, which is encouraged for persons with hypertension
- ensuring that persons with
- hypertension are screened for diabetes
- diabetes are screened for hypertension
- assessment and management overall of cardiovascular risk in all persons with hypertension including the risks of
- abdominal obesity
- blood sugar disorders
- cholesterol disorders
- physical inactivity
- smoking
- unhealthy eating
- sustained lifestyle modification as the basis for prevention and management of hypertension and cardiovascular disease, with particular emphasis on plans for
- achieving individual targets for blood pressure
- controlling weight
- DASH guide for eating
- exercising
- reducing stress
- quitting smoking
- using optimally medications in conjunction with lifestyle changes, attention to causal factors, and treatment of associated medical conditions and comorbidities to bring blood pressure below the targets in the Tables: CDHO Advice for Adults Incorporating Hypertension Canada/CHEP Recommendations and Oral Health-Specific Resources
- recognition of hypertensive urgencies and emergencies, such as asymptomatic diastolic blood pressure at or above 120 to 130 mm Hg, which require immediate medical referral
- when controlled by reaching and maintaining target levels results in substantial reduction of risk of premature death associated with
- coronary artery or other vascular disease
- heart attack
- heart failure
- stroke.
Prognosis of hypertension
Hypertension
- deaths in Ontario measured as rates of deaths among persons diagnosed with hypertension decreased by 15.5 percent between 1995 and 2005
- diagnoses in Ontario increased by 60 percent between 1995 and 2005 and may be continuing to do so because
- persons with the diagnosis of hypertension are living longer
- awareness of hypertension as a risk has increased
- treatment and prevention have improved in effectiveness
- diagnostic criteria has evolved.
Social considerations of hypertension
Hypertension is associated with unfavourable social factors associated with unfavourable lifestyles, which are all associated with hypertension in susceptible individuals, and which
- increase tendencies to abdominal obesity
- include
- less-than-healthy diet
- insufficient exercise
- smoking
- psychosocial stress.
Multimedia and images
Comorbidity, complications and associated conditions
Comorbid conditions are those which co-exist with hypertension but which are not believed to be caused by it. Complications and associated conditions are those that may have some link with it. Distinguishing among comorbid conditions, complications and associated conditions may be difficult in clinical practice.
Comorbid conditions, complications and associated conditions for hypertension are as follows.
Hypertension
- when untreated may be associated with atherosclerosis, leading to increased risk of coronary artery disease because high blood pressure puts added force against the artery walls which, over time, may damage the arteries and increase the likelihood of narrowing and plaque build-up, which
- limits or blocks the flow of blood to the heart muscle and deprives it of oxygen
- also leads to
- the formation of small blood clots
- blockage of blood vessels, causing
- clot-related stroke
- heart attack
- rupture of blood vessels, as in massive hemorrhagic stroke
- leaking or rupture of blood vessels in the eye.
- occurs in roughly one-third of the general population, but its occurrence reaches 75 percent in persons with comorbidities that carry cardiovascular risk, especially
- chronic kidney disease
- coronary artery disease
- diabetes, which is subject to a risk of coronary-artery events equal to the risk of these events with established cardiovascular disease
- peripheral artery disease
- stroke.
- has an extensive range of comorbidities, complications and associated conditions, which include
- anxiety
- bipolar disorder
- congestive heart failure
- dementia
- depression, in which blood pressure may be increased by the drugs used to treat depression rather than the depression itself
- heart disease affecting the left ventricle
- hypertensive retinopathy
- mixed vascular dementia and dementia of the Alzheimer’s type
- vascular dementia.
Oral health considerations
Resources consulted
- College of Dental Hygienists of Ontario: Hypertension in Children & Adolescents Fact Sheet
- Gum Disease (Periodontal Disease) – Medline Plus
- Hypertension Canada (formerly CHEP) Guidelines
- The 2016 CHEP Recommendations for the Management of Hypertension state that all Canadian adults should have their blood pressure assessed at all appropriate clinical visits. Reinforced by the 2018 and 2020 Hypertension Canada Guidelines for Diagnosis, Risk Assessment, Prevention, and Treatment of Hypertension in Adults and Children, automated electronic (oscillometric) measurement methods are preferred over manual and auscultatory measurement in adults to determine cardiovascular risk and monitor antihypertensive treatment.
- The 2020 Hypertension Canada Guidelines state that children ≥ 3 years of age should have their blood pressure regularly measured. The auscultatory method of blood pressure measurement is preferred for children over automated methods.
- As healthcare professionals, dental hygienists who have been specifically trained to measure blood pressure accurately have
- appropriate visits with their patients/clients
- an important role in determining cardiovascular risk arising from the effects of
- hypertension on the safety of the Procedures
- oral health conditions on hypertension and its comorbidities, complications and associated conditions
- some role in monitoring antihypertensive treatment, with particular reference to
- oral side effects of medications
- lifestyle factors.
- Dental hygiene has prevention as one of its professional purposes, which positions dental hygienists as healthcare professionals with particular contributions to make to the prevention of hypertension, a major preoccupation of public policy and public health in Canada.
- In their interpretations of blood pressure measurements taken in dental hygiene settings dental hygienists should be aware of the particular constraints inherent in the Hypertension Canada/CHEP Recommendations, which may require patterns of practice that lie outside the duties normally expected of dental hygienists, such as the Hypertension Canada/CHEP recommendations for
- reliance on averages of repeated blood pressure measurements as the basis for
- diagnosis and assessment of hypertension
- modifications to medications regimes
- sequences of office visits
- specifically related to assessments of hypertension
- at which the blood pressure measurements are made and averaged over some or all of the visits
- repeated follow-up of hypertension-specific visits.
- reliance on averages of repeated blood pressure measurements as the basis for
- The Tables: CDHO Advice for Adults Incorporating Hypertension Canada/CHEP Recommendations and Oral Health-Specific Resources draw on the Hypertension Canada/CHEP recommendations, apply these to single dental hygiene visits, and provide advice to dental hygienists relative to the situations identified in the table.
- Tables 3, 4, and 5 draw on Hypertension Canada recommendations for blood pressure measurement and hypertension criteria for children and adolescents. Table 6 is a simplified table for pediatric screening blood pressure values requiring medical evaluation, drawing on reputable American sources. As adjuncts to Table 4, weblinks to tables and a calculator are provided for determination of normative data for blood pressure values in children/adolescents.
- The role of the dental hygienist in relation to hypertension and its comorbidities, complications and associated conditions includes
- responding with an emergency 911 call to signs and symptoms
- indicative of possible hypertensive crisis
- indicative of possible malignant hypertension
- convulsions (seizures)
- affecting a pregnant woman
- indicative of a serious condition in need of prompt attention
- using clinical judgment about the need for routine blood pressure measurements for individual patients/clients, although such measurements
- relative to various risk factors for hypertension are a necessary preliminary precaution for the Procedures and other aspects of dental hygiene care
- may enable dental hygienists to promote oral and general health for some patients/clients through healthy lifestyles and compliance with medications
- measuring blood pressure preparatory to the Procedures when the patient/client
- exhibits severe periodontal disease, which may be a risk factor for hypertension and cardiovascular disease
- is diabetic
- is pregnant
- provides a medications history of use of anti-hypertensive medications
- provides a medical history suggestive of
- hypertension
- chronic kidney disease
- coronary artery disease
- stroke
- provides a medical history or displays an outward appearance suggestive of risk factors of hypertension, such as
- abdominal obesity
- problems with blood cholesterol
- physical inactivity
- smoking
- unhealthy eating
- is known to have comorbid conditions that may affect hypertension, such as
- cerebrovascular disease
- dementia
- stroke
- vascular dementia
- mixed vascular dementia and dementia of the Alzheimer’s type
- anxiety, depression or bipolar disorder
- hypertensive retinopathy
- heart disease affecting the left ventricle
- congestive heart failure
- cerebrovascular disease
- giving special consideration to elderly, hypertensive patients/clients relative to
- avoiding anxiety and pain
- arranging for control of blood pressure before oral healthcare begins
- seeking medical opinion relative to persistently high blood pressure readings
- acting on a marked rise in blood pressure during oral healthcare, including
- interrupting treatment
- placing the patient in the supine position to allow rest
- repeating the blood pressure reading after five minutes
- acting according to the advice in the Tables: CDHO Advice for Adults Incorporating Hypertension Canada/CHEP Recommendations and Oral Health-Specific Resources if the blood pressure remains high
- giving special consideration to children with hypertension, for whom invasive dental procedures may signal need for particular precautions
- before treatment by
- assessing the medical and family history of hypertension and medications
- reducing stressors that could cause the blood pressure to rise
- measuring base-line blood pressure
- referring for medical consultation if the blood pressure appears uncontrolled
- during treatment, where indicated by base-line blood pressure measurements and medical advice, by
- monitoring blood pressure
- avoiding local anesthetics with vasoconstrictors
- ensuring pain control to maintain stability of blood pressure
- evaluating xerostomia especially related to diuretics; if present, considering fluoride supplements or artificial saliva on a daily basis
- assessing gingival overgrowth associated with calcium channel blockers
- after treatment, where indicated by base-line blood pressure measurements and medical advice, by
- monitoring blood pressure and, if appropriate, vital signs
- limiting non-steroid anti-inflammatory drugs (NSAIDS) to no more than a ten-day course.
- before treatment by
- responding with an emergency 911 call to signs and symptoms
- Other oral health considerations relating to blood pressure and its treatment include
- prolonged use of nonsteroidal anti-inflammatory agents (NSAIDs), which reduces the effectiveness of various antihypertensive medications: patients/clients should generally be given no more than a ten-day course.
- orthostatic hypotension, which
- is a risk for persons, especially older persons, taking multiple medications for hypertension
- occurs if the person attempts to quickly stand upright after a prolonged period reclining or in the supine position
- may cause syncope with the risk of falling and associated injury
- is avoided by enabling the patient/client to sit upright for a few minutes after completion of the oral healthcare procedure
- xerostomia
- is associated with various antihypertensive medications, such as
- alpha blockers
- angiotensin-converting enzyme inhibitors
- beta blockers
- calcium channel blockers
- diuretics
- may cause
- candidiasis
- caries
- difficulties with mastication, swallowing and speech
- oral burning
- sometimes self-corrects through the adaptation of salivary function, though may also require
- change in medication
- enhanced self-care by the patient/client, such as
- frequent sips of water
- moisturizing gels
- sugarless hard candy, sugarless mints or gums
- minimization of caffeine intake
- avoiding alcohol-containing mouth rinses
- direct treatment involving parasympathomimetic agents such as
- application or increased application of fluoride to combat the potential for caries
- is associated with various antihypertensive medications, such as
- gingival overgrowth, which
- may be caused by calcium channel blockers, leading to pain, gingival bleeding and difficulty with mastication
- is prevented or reduced by rigorous oral hygiene
- may be reversible with change in anti-hypertensive medication
- may require gingivectomy or gingivoplasty or both for extensive overgrowth
- lichenoid reactions, which
- closely resemble lichen planus
- are caused by various cardiovascular medications, such as
- angiotensin-converting enzyme inhibitors
- beta blockers
- diuretics
- are treated
- in the first approach by change of medication; if the lichenoid lesions are associated with the particular antihypertensive, they will resolve when it is changed
- if the first approach is unsuccessful, lichenoid reactions may be treated with topical corticosteroids.
- effects of angiotensin-converting enzyme inhibitors such as cough, loss of taste and, reportedly, a burning sensation described as ‘scalded mouth’ syndrome
- epinephrine in local anesthetics and interaction
- with some beta-blockers, which
- may result in a reduction in cardiac output and for this reason has in some oral healthcare practice led to the avoidance of epinephrine in local anesthetic solutions, but systematic review in 2004 by the American Heart Association, see p. 1237 concluded that, although adverse events may occur during dental procedures in patients with uncontrolled hypertension, the use of epinephrine had minimal effect
- may be administered to an individual patient/client in a single session
- of not more than two or three cartridges of anesthetic with 1:100,000 epinephrine
- with careful administration, and frequent aspiration and monitoring of vital signs
- non-potassium-sparing diuretics, which may cause potassium levels to decrease, resulting in cardiac dysrhythmia.
- with some beta-blockers, which
MEDICATIONS SUMMARY
Sourcing medications information
- Adverse effect database
- Health Canada’s Marketed Health Products Directorate (MedEffect Canada) toll-free 1-866-234-2345
- Health Canada’s Drug Product Database
- Specialized organizations
- US National Library of Medicine and the National Institutes of Health Medline Plus Drug Information
- WebMD
- Mayo Clinic (regarding central acting antihypertensive medications)
- Mayo Clinic (regarding direct vasodilator antihypertensive medications)
- Medications considerations
- All medications have potential side effects whether taken alone or in combination with other prescription medications, or as over-the-counter (OTC) or herbal medications.
- Information on herbals and supplements
- Complementary and alternative medicine
Types of medications
Often taken in combinations, antihypertensive medications comprise
- Diuretics, which remove excess sodium and fluid to reduce the amount of water and therefore the volume of fluid circulating in the blood; these include
- amiloride and hydrochloride (Moduretic®)
- bumetanide (Bumex®)
- chlorthalidone (Hygroton®, Thalitone®)
- ethacrynic acid (Edecrin®)
- furosemide (Lasix®)
- hydrochlorothiazide (HydroDiuril®, Microzide®)
- indapamide (Lozol®)
- metolazone (Mykrox®, Zaroxolyn®)
- spironolactone (Aldactone®)
- torsemide (Demadex Oral®)
- triamterene (Dyrenium®)
- Beta blockers, which block the effects of adrenaline, thereby reducing the heart rate and the force of the heart pumping action; these include
- acebutolol (Sectral®)
- atenolol (Tenormin®)
- betaxolol (Kerlone®)
- bisoprolol (Zebeta®)
- carvedilol (Coreg®)
- labetalol (Normodyne®, Trandate®)
- metoprolol (Lopressor®)
- nadolol (Corgard®)
- penbutolol (Levatol®)
- propranolol (Inderal®)
- timolol (Blocadren®)
- Calcium channel blockers, which inhibit blood-vessel constriction by blocking calcium from entering the cells of the heart and blood vessel, or by reducing the force with which the blood is pumped, thereby reducing the blood pressure; these include
- amlodipine (Norvasc®)
- diltiazem (Cardizem®)
- felodipine (Plendil®)
- isradipine (DynaCirc®)
- nicardipine (Cardene®)
- nifedipine (Adalat®, Nifedical®, Procardia®)
- nisoldipine (Sular®)
- verapamil (Isoptin®)
- Angiotensin-converting enzyme inhibitors (ACEIs), which inhibit blood-vessel constriction by blocking production of angiotensin II, a substance that constricts blood vessels; these include the following
- benazepril (Lotensin®)
- captopril (Capoten®)
- enalapril (Vasotec®)
- fosinopril (Monopril®)
- lisinopril (Prinivil®, Zestril®)
- moexipril (Univasc®)
- quinapril (Accupril®)
- ramipril (Altace®)
- trandolapril (Mavik®)
- Angiotensin II receptor blockers (ARBs), which are similar to ACE inhibitors, but block angiotensin’s narrowing action on blood vessels; these include
- azilsartan (Edarbi®)
- candesartan (Atacand®)
- eprosartan (Teveten®)
- irbesartan (Avapro®)
- losartan (Cozaar®)
- olmesartan (Benicar®)
- telmisartan (Micardis®)
- valsartan (Diovan®)
- Alpha blockers, which relax certain muscles and combat the constricting effect of noradrenaline on blood vessels; these include
- alfuzosin (Uroxatral®)
- doxazosin (Cardura®)
- prazosin (Minipress®)
- tamsulosin (Flomax®)
- terazosin (Hytrin®)
- Central acting agents, which block signals from the brain that increase heart rate and narrow blood vessels; these include
- clonidine (Catapres®, Kapvay®)
- guanfacine (Intuniv®, Tenex®)
- methyldopa (Aldomet®)
- Direct vasodilators, which work directly on vessel walls and are generally used only when other medications fail to adequately control blood pressure; these include
- hydralazine (Alpresoline®, Dralzine®)
- minoxidil (Loniten®)
Side effects of medications
See the links above to the specific medications.
THE MEDICAL AND MEDICATIONS HISTORY
The dental hygienist in taking the medical and medications history-taking should
- focus on screening the patient/client prior to treatment decision relative to
- key symptoms
- medications considerations
- contraindications
- complications
- comorbidities
- associated conditions
- explore the need for advice from the primary or specialized care provider(s)
- inquire about
- pointers in the history of significance to hypertension, such as the medications history
- symptoms indicative of inadequate control of hypertension, such as frequent changes in medications and doses
- the patient/client’s understanding and acceptance of the need for oral healthcare
- medications considerations, including over-the-counter medications, herbals and supplements
- problems with previous dental/dental hygiene care
- problems with infections generally and specifically associated with dental/dental hygiene care
- the patient/client’s current state of health
- how the patient/client’s current symptoms relate to
- oral health
- health generally
- recent changes in the patient/client’s condition.
IDENTIFYING AND CONTACTING THE MOST APPROPRIATE HEALTHCARE PROVIDER(S) FOR ADVICE
Identifying and contacting the most appropriate healthcare provider(s) from whom to obtain medical or other advice pertinent to a particular patient/client
The dental hygienist should
- record the name of the physician/primary care provider most closely associated with the patient/client’s healthcare, and the telephone number
- obtain from the patient/client or parent/guardian written, informed consent to contact the identified physician/primary healthcare provider
- use a consent/medical consultation form, and be prepared to securely send the form to the provider
- include on the form a standardized statement of the Procedures proposed, with a request for advice on proceeding or not at the particular time, and any precautions to be observed.
UNDERSTANDING AND TAKING APPROPRIATE PRECAUTIONS
Infection Control
Dental hygienists are required to keep their practices current with infection control policies and procedures, especially in relation to
- the CDHO’s Infection Prevention and Control Guidelines (2022)
- relevant occupational health and safety legislative requirements
- relevant public health legislative requirements
- best practices or other protocols specific to the medical condition of the patient/client.
DECIDING WHEN AND WHEN NOT TO INITIATE THE PROCEDURES PROPOSED
- There is no contraindication to the Procedures unless SBP4≥ 180 mm Hg and/or DBP5≥ 110 mm Hg OR there are warning symptoms/signs in the hypertensive patient/client at lower levels of BP; e.g., severe headache, blurred vision, shortness of breath, nosebleeds, nausea/vomiting, chest pain, or seizures. In patients/clients with risk factors such as myocardial infarction, angina pectoris, high coronary disease risk, recurrent stroke, diabetes mellitus, and renal disease, invasive procedures should not be performed if SBP ≥ 160 mm Hg and/or DBP ≥ 100 mm Hg. (See attached tables for further details.)
- With an otherwise healthy patient/client whose hypertension is under control and whose treatment is proceeding normally, the dental hygienist should implement the Procedures, though these may be postponed pending medical advice, which may be required if the patient/client has
- symptoms or signs of exacerbation of the hypertension
- comorbidity, complication or an associated condition of hypertension
- not recently or ever sought and received medical advice relative to oral healthcare procedures
- recently changed significant medications, under medical advice or otherwise
- recently experienced changes in his/her medical condition such as medication or other side effects of treatment
- is deeply concerned about any aspect of his or her medical condition.
DEALING WITH ANY ADVERSE EVENTS ARISING DURING THE PROCEDURES
Dental hygienists are required to initiate emergency protocols as required by the College of Dental Hygienists of Ontario’s Standards of Practice, and as appropriate for the condition of the patient/client.
First-aid provisions and responses as required for current certification in first aid.
RECORD KEEPING
Subject to Ontario Regulation 9/08 Part III.1, Records, in particular S 12.1 (1) and (2) for a patient/client with a history of hypertension, the dental hygienist should specifically record
- a summary of the medical and medications history
- any advice received from the physician/primary care provider relative to the patient/client’s condition
- the decision made by the dental hygienist, with reasons
- compliance with the precautions required
- all Procedure(s) used
- any advice given to the patient/client.
ADVISING THE PATIENT/CLIENT
The dental hygienist should
- urge the patient/client to alert any healthcare professional who proposes any intervention or test
- that he or she has a history of hypertension
- to the medications he or she is taking
- should discuss, as appropriate
- the importance of the patient/client’s
- self-checking the mouth regularly for new signs or symptoms
- reporting to the appropriate healthcare provider any changes in the mouth
- the need for regular oral health examinations and preventive oral healthcare
- oral self-care including information about
- choice of toothpaste
- tooth-brushing techniques and related devices
- dental flossing
- mouth rinses
- management of a dry mouth
- the importance of an appropriate diet in the maintenance of oral health
- for persons at an advanced stage of a disease or debilitation
- regimens for oral hygiene as a component of supportive care and palliative care
- scheduling and duration of appointments to minimize stress and fatigue
- comfort level while reclining, and stress and anxiety related to the Procedures
- medication side effects such as dry mouth, and recommend treatment
- mouth ulcers and other conditions of the mouth relating to hypertension, comorbidities, complications or associated conditions, medications or diet
- pain management, with particular reference to the use of NSAIDs.
- the importance of the patient/client’s
BENEFITS/HARMS OF IMPLEMENTING THE RECOMMENDATIONS
POTENTIAL BENEFITS
- Promoting health through oral hygiene for persons who have hypertension or who are receiving treatment for hypertension.
- Reducing the adverse effects, such as by
- early detection of asymptomatic hypertension
- generally increasing the comfort level of persons in the course of dental hygiene interventions
- using appropriate techniques of communication
- providing advice on scheduling and duration of appointments.
- Reducing the risk that oral health needs are unmet.
POTENTIAL HARMS
- Causing stress and anxiety, and overlooking a hypertensive emergency.
- Disturbing the normal dietary and medications routine of a person with hypertension.
- Performing the Procedures at an inappropriate time, such as
- in the absence of adequate precautions before, during and after the Procedures
- in the presence of complications for which prior medical advice is required
- in the presence of acute oral infection without prior medical advice.
- Disturbing the normal dietary and medications routine of a person with hypertension.
- Inappropriate management of pain or medication.
CONTRAINDICATIONS
CONTRAINDICATIONS IN REGULATIONS
Identified in the Dental Hygiene Act, 1991 – O. Reg. 218/94 Part III
ORIGINALLY DEVELOPED
2009-10-27
DATE OF LAST REVIEW
2011-11-01; 2014-04-10; 2014-05-02; 2015-02-24; 2016-08-22; 2017-07-18; 2019-08-13; 2020-06-04; 2021-08-25; 2022-05-22; 2023-04-18
ADVISORY DEVELOPER(S)
College of Dental Hygienists of Ontario, regulatory body
Greyhead Associates, medical information service specialists
SOURCE(S) OF FUNDING
College of Dental Hygienists of Ontario
ADVISORY COMITTEE
College of Dental Hygienists of Ontario, Practice Advisors
COMPOSITION OF GROUP THAT AUTHORED THE ADVISORY
Dr Gordon Atherley
O StJ , MB ChB, DIH, MD, MFCM (Royal College of Physicians, UK), FFOM (Royal College of Physicians, UK), FACOM (American College of Occupational Medicine), LLD (hc), FRSA
Dr Kevin Glasgow
MD, MHSc, MBA, DTM&H, CHE, CCFP, DABPM, LFACHE, FCFP, FACPM, FRCPC
Lisa Taylor
RDH, BA, MEd
Robert Farinaccia
RDH, BSc
Roula Anastasopoulos
RDH, BEd
Giulia Galloro
RDH, BSc(DH)
Kyle Fraser
RDH, BComm, BEd, MEd
Carolle Lepage
RDH, BEd
ACKNOWLEDGEMENTS
The College of Dental Hygienists of Ontario gratefully acknowledges the Template of Guideline Attributes, on which this advisory is modelled, of The National Guideline Clearinghouse™ (NGC), sponsored by the Agency for Healthcare Research and Quality (AHRQ), U.S. Department of Health and Human Services.
Denise Lalande
Final layout and proofreading
COPYRIGHT STATEMENT(S)
© 2009, 2011, 2014–2023 College of Dental Hygienists of Ontario
The tables that follow are intended only as guides to help inform decision-making. The dental hygienist must also consider the current clinical status of the patient/client in the office. Patients/clients with high blood pressure who have signs/symptoms such as severe headache, blurred vision, shortness of breath, nosebleeds, nausea/vomiting, chest pain, or seizures, should be referred to a physician for immediate evaluation. Furthermore, the dental hygienist should compare current BP reading with previous readings. A person who typically has low or normal blood pressure who now has unexpectedly elevated blood pressure may be more worrisome in the short-term than a person who habitually has high blood pressure.
Where the tables advise that non-invasive procedures (e.g., oral hygiene instruction, fitting a mouth guard, and taking an impression) +/- invasive procedures (i.e., scaling teeth and root planing, including curetting surrounding tissue) may be undertaken, the dental hygienist should consider the individual circumstances of each patient/client. Specific procedures (be they non-invasive or invasive) should be avoided if the dental hygienist believes they could cause stress/anxiety resulting in a sudden, acute elevation in blood pressure. This individual consideration of stress/anxiety is particularly important for patients/clients with pre-existing high blood pressure. If in doubt, the dental hygienist should defer the procedure(s) pending medical evaluation.
CDHO Advice for Adults Incorporating Hypertension Canada/CHEP Recommendations and Oral Health-Specific Sources
Table 1****This table is to be used if an adult patient/client presents WITHOUT A HISTORY of other risk factors such as history of myocardial infarction, angina pectoris, high coronary disease risk, recurrent stroke, diabetes mellitus, or renal disease.
Note: AOBP = automated office blood pressure (i.e., BP obtained via an automated device that can take a series of oscillometric measurements, with patient/client unattended in a private area); non-AOBP = non-automated office blood pressure (includes BP obtained via electronic upper arm device with the provider in the room) [BP readings in Table 1 refer to non-AOBP unless otherwise indicated.]
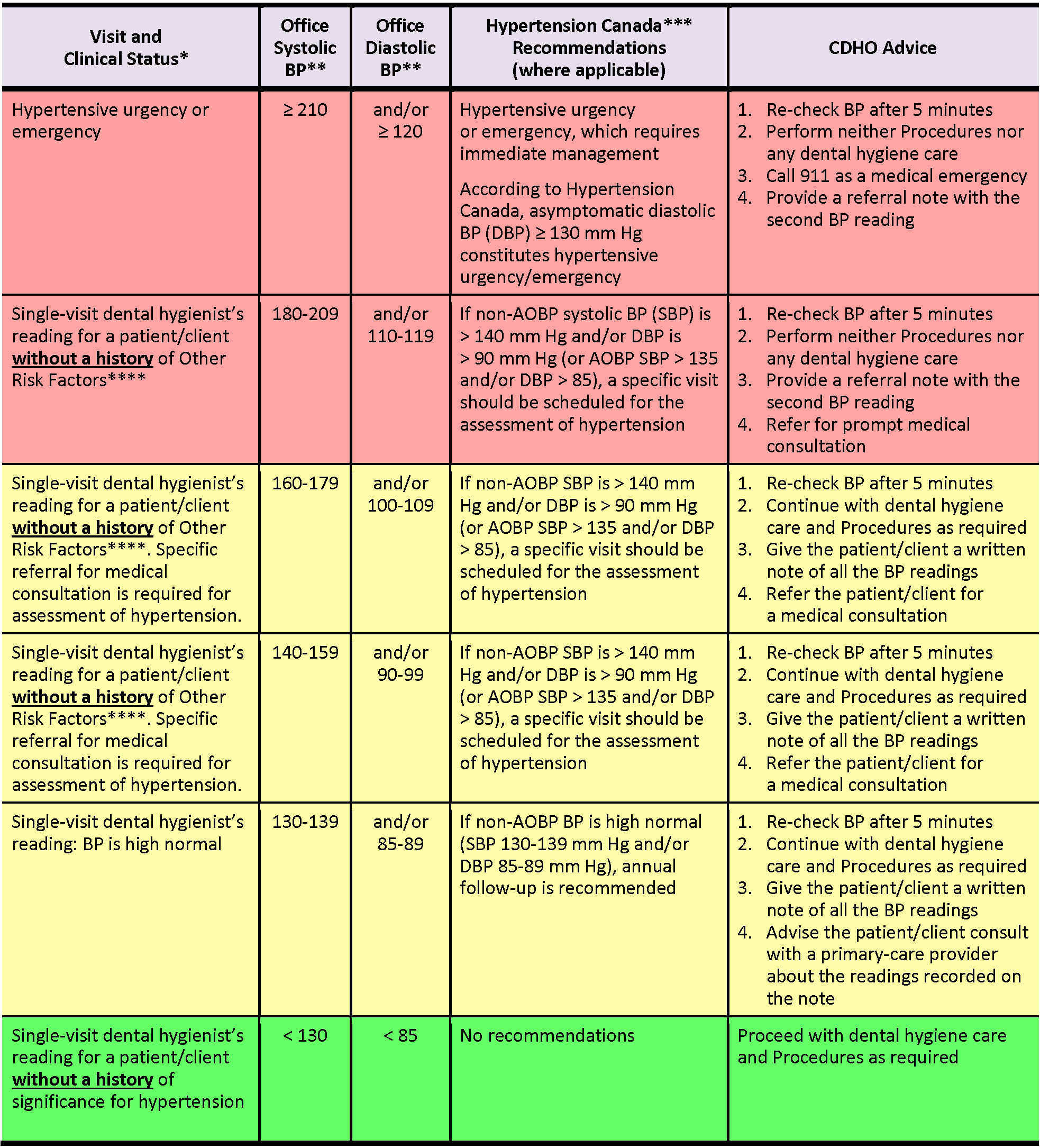
Table 2 ****This table is to be used if an adult patient/client presents WITH A HISTORY of risk factors such as history of myocardial infarction, angina pectoris, high coronary disease risk, recurrent stroke, diabetes mellitus, or renal disease.
Note: AOBP = automated office blood pressure; (i.e., BP obtained via an automated device that can take a series of oscillometric measurements, with patient/client unattended in a private area); non-AOBP = non-automated office blood pressure (includes BP obtained via electronic upper arm device with the provider in the room) [BP readings in Table 2 refer to non-AOBP unless otherwise indicated.]
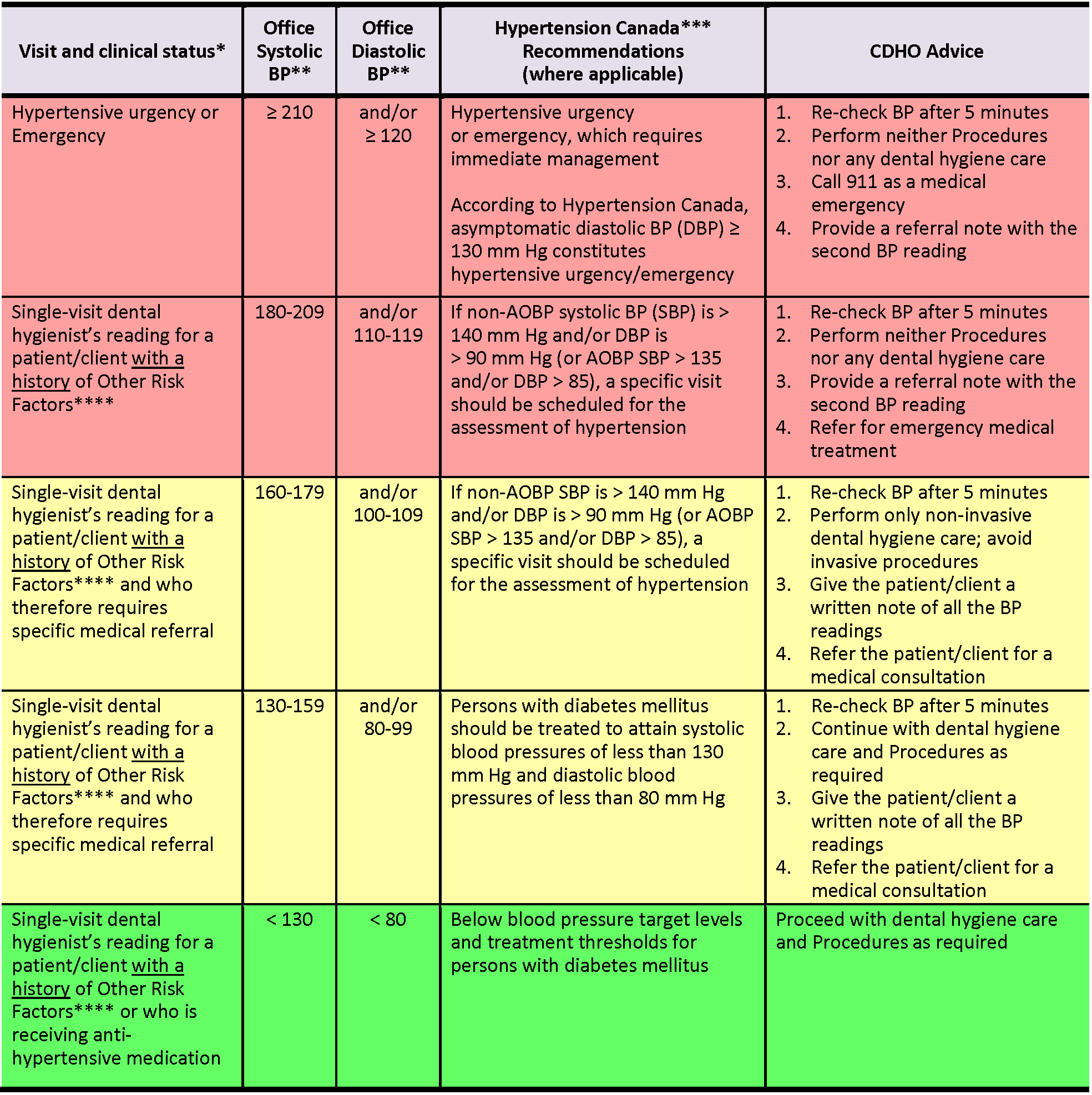
* Assumes that the measurement is repeated at least once over a period of five minutes or more, with the patient/client at rest
** mm Hg (≥ means ‘equal to or more than’; < means ‘less than’; ≤ means ‘equal to or less than’)
*** CHEP 2016 Guidelines stated that target systolic BP in the very elderly (age ≥ 80 years) is < 150 mm Hg, rather than < 140 mm Hg in other, non-diabetic adults. However, superseding this, Hypertension Canada’s 2017 Guidelines (formerly CHEP Guidelines) state that target systolic BP is ≤ 120 mm Hg for high-risk patients/clients, which includes persons age ≥ 75 years.
**** Other Risk Factors: history of myocardial infarction, angina pectoris, high coronary disease risk, recurrent stroke, diabetes mellitus, renal disease
Table 3: Standard approach for BP measurement in children
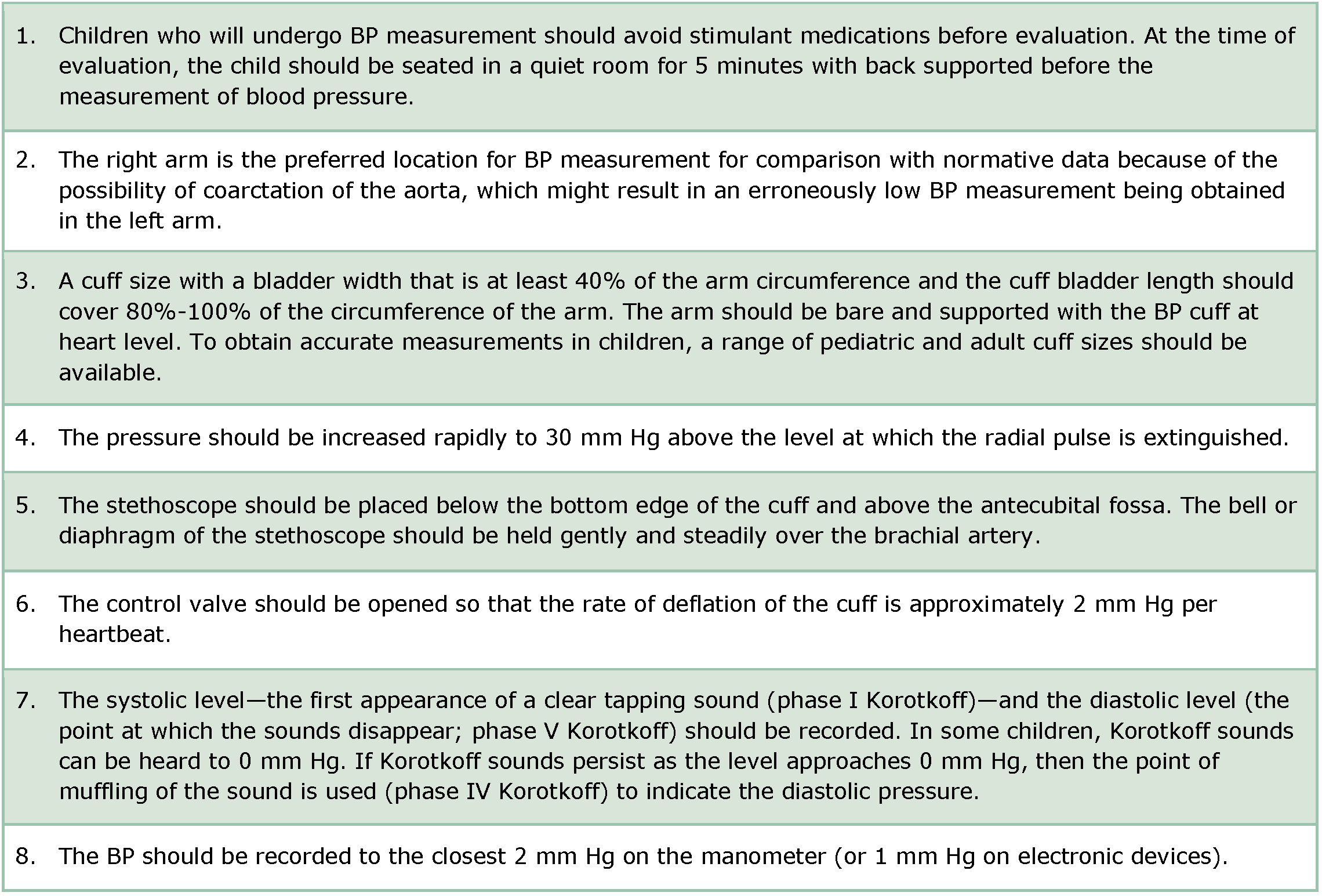
Adapted from: Hypertension Canada’s 2020 Guidelines for Diagnosis, Risk Assessment, Prevention, and Treatment of Hypertension in Adults and Children
Table 4: Determining normative data for blood pressure values in children
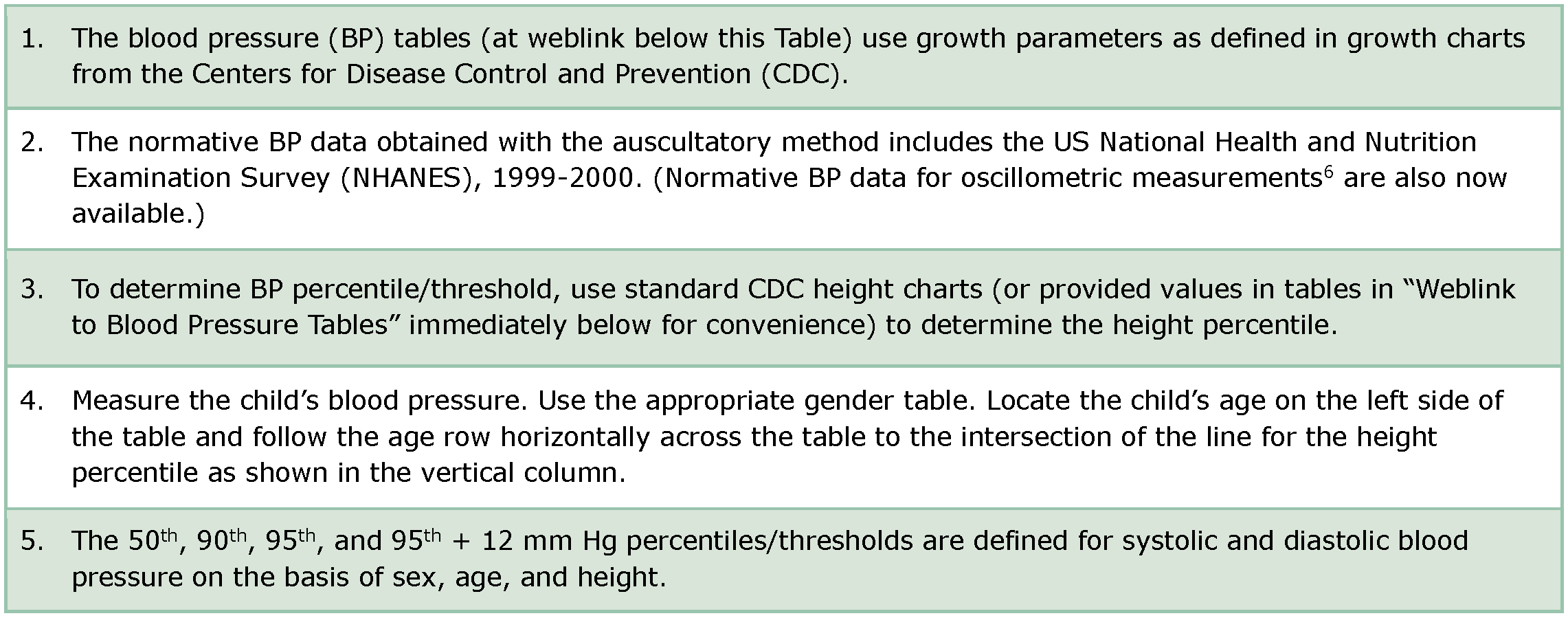
Adapted from: 1/ Hypertension Canada’s 2020 Guidelines for Diagnosis, Risk Assessment, Prevention, and Treatment of Hypertension in Adults and Children. 2/ Flynn JT, Kaelber DC, Baker-Smith CM, et al. Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents. Pediatrics. 2017 Sep;140(3):e20171904. doi: 10.1542/peds.2017-1904. Epub 2017 Aug 21.
Weblink to Blood Pressure Tables for determination of normative data for blood pressure values in children/adolescents: https://pediatrics.aappublications.org/content/140/3/e20171904 (Refer to article’s Table 4 for BP Levels for Boys by Age and Height Percentile; Refer to article’s Table 5 for BP Levels for Girls by Age and Height Percentile)
Weblink to Calculator for determination of normative data for blood pressure values in children/adolescents: https://www.bcm.edu/bodycomplab/BPappZjs/BPvAgeAPPz.html. (Note: While this calculator can be used to determine percentiles for SBP and DBP by sex/age/height, the included American definitions of elevated blood pressure and hypertension differ somewhat from Hypertension Canada’s 2020 guidelines.)
Table 5: Criteria for Diagnosis of Hypertension in Children and Adolescents
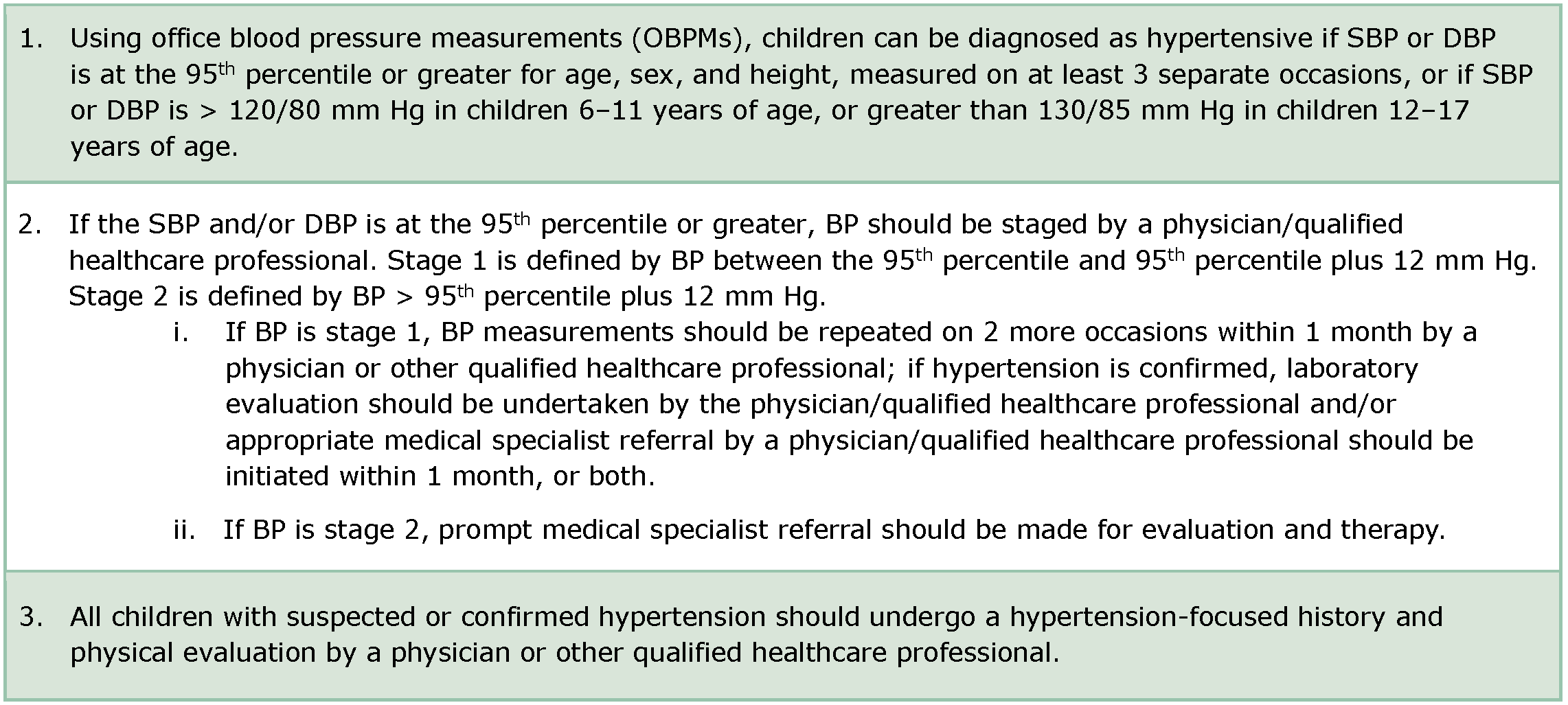
Adapted from: Hypertension Canada’s 2020 Guidelines for Diagnosis, Risk Assessment, Prevention, and Treatment of Hypertension in Adults and Children
Table 6: Simplified Table for Screening Blood Pressure Values Requiring Further Medical Evaluation
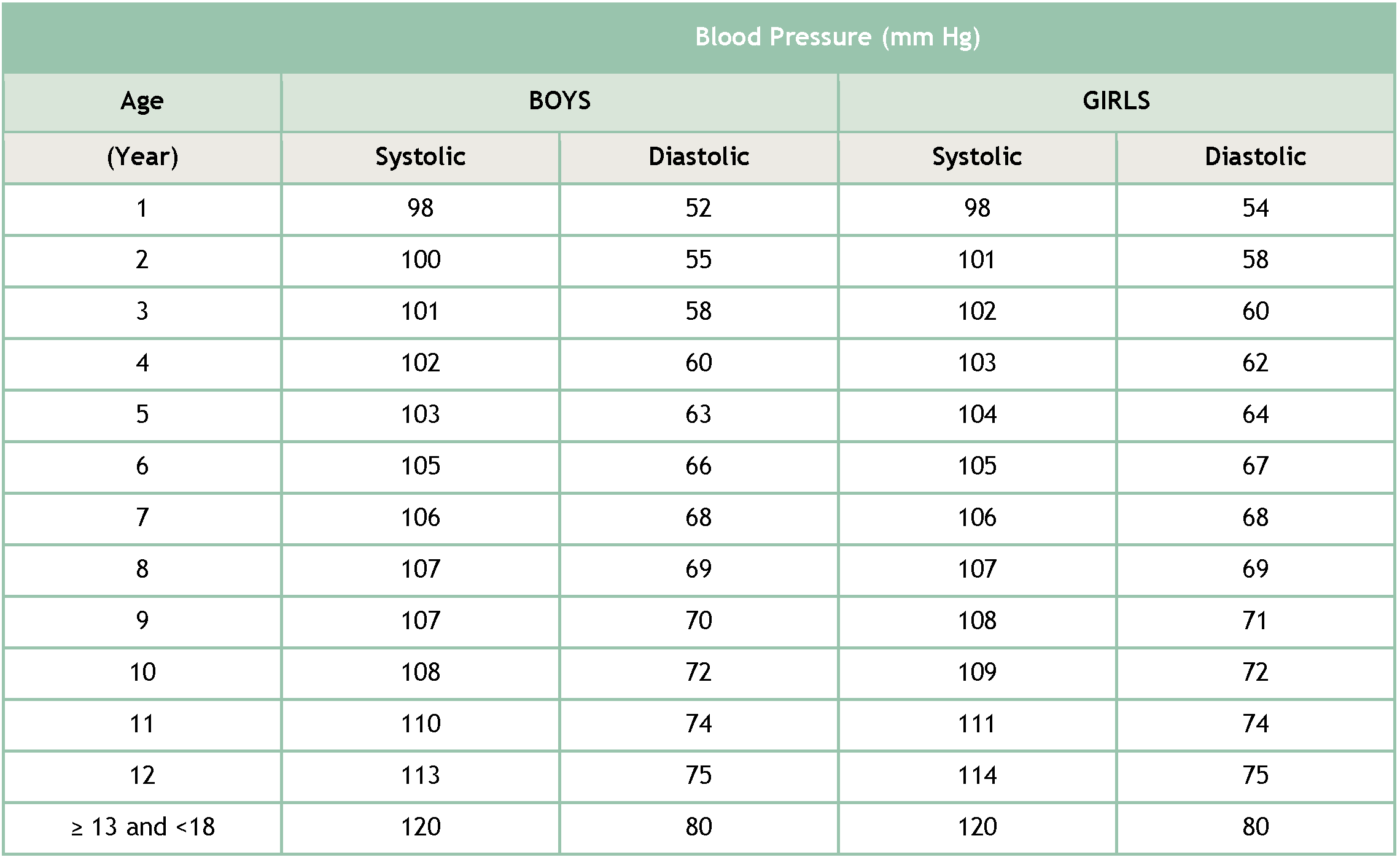
Note: This simplified table for initial blood pressure (BP) screening is based on the 90th percentile BP for sex and age for children at the 5th percentile of height. It should not be used to diagnose elevated BP or hypertension by itself, because SBP and DBP cut-offs in complete BP tables may be as much as 9mm Hg higher depending on a child’s age and height.
Adapted from: 1/ Bowen DM (ed.) and Pieren JA (ed.). Darby and Walsh Dental Hygiene: Theory and Practice (5th edition). St. Louis: Elsevier; 2020. 2/ Flynn JT, Kaelber DC, Baker-Smith CM, et al. Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents. Pediatrics. 2017 Sep;140(3):e20171904. doi: 10.1542/peds.2017-1904. Epub 2017 Aug 21.
Sources
- College of Dental Hygienists of Ontario
https://cdho.org/factsheets/hypertension-in-adults/ (Hypertension in Adults) - College of Dental Hygienists of Ontario
https://cdho.org/factsheets/hypertension-in-children-adolescents/ - Farinaccia R. Hypertension 101. Milestones July 2013: 20–21.
- Farinaccia R. Blood Pressure Guidelines – Updated for 2014. Milestones July 2014: 12–13.
- College of Dental Hygienists of Ontario. Blood Pressure Protocol. Milestones March 2015: 9
- Zahedi S and Marciniak R. The Hypertensive Patient (A review of the latest Joint National Committee on Prevention, Detection, Evaluation and Treatment of Hypertension as it applies to the dentist). Oral Health 2012-02-01.
https://www.oralhealthgroup.com/features/the-hypertensive-patient/ - Hypertension Canada https://guidelines.hypertension.ca
- Hypertension Canada’s 2020-2022 Hypertension Highlights: A Practical Guide informed by the Hypertension Canada Guidelines for the Prevention, Diagnosis, Risk Assessment, and Treatment of Hypertension
https://hypertension.ca/wp-content/uploads/2020/10/2020-22-HT-Guidelines-E-WEB_v3b.pdf - Hypertension Canada’s 2020 Hypertension Highlights: A Practical Guide informed by the Hypertension Canada Guidelines for the Diagnosis, Risk Assessment, Prevention, and Treatment of Hypertension
https://hypertension.ca/wp-content/uploads/2018/07/Hypertension-Guidelines-English-2018-Web.pdf - Hypertension Canada’s 2020 Comprehensive Guidelines for Diagnosis, Risk Assessment, Prevention, and Treatment of Hypertension in Adults and Children
https://www.onlinecjc.ca/article/S0828-282X(20)30191-4/fulltext - Hypertension Canada’s 2018 Guidelines for Diagnosis, Risk Assessment, Prevention, and Treatment of Hypertension in Adults and Children
https://www.onlinecjc.ca/article/S0828-282X(18)30183-1/fulltext - Hypertension Canada’s 2017 Guidelines for the Management of Hypertension
https://www.hypertension.ca/images/CHEP_2017/HTN_Whats_New_2017_EN.pdf - Hypertension Canada’s 2017 Guidelines for Diagnosis, Risk Assessment, Prevention, and Treatment of Hypertension in Adults
http://www.onlinecjc.ca/article/S0828-282X(17)30110-1/pdf - Canadian Hypertension Education Program’s 2016 Guidelines
https://www.onlinecjc.ca/article/S0828-282X(16)00192-6/fulltext - Government of Canada
https://www.canada.ca/en/public-health/services/chronic-diseases/cardiovascular-disease/hypertension.html - Heart & Stroke Foundation https://www.heartandstroke.ca/-/media/pdf-files/canada/health-information-catalogue/en-get-your-blood-pressure-under-control-v21-web.ashx?la=en&hash=20493566724F3F87387717A720D49F60521C1CF2
- American College of Cardiology/American Heart Association’s 2017 Hypertension Guidelines and related commentary
https://www.acc.org/latest-in-cardiology/articles/2019/04/04/12/50/similarities-and-differences-between-the-2017-acc-aha-bp-guideline-and-2017-ada-diabetes-and-htn-position-statement - American College of Cardiology/American Heart Association’s 2019 Guideline on the Prevention of Cardiovascular Disease
https://www.acc.org/latest-in-cardiology/ten-points-to-remember/2019/03/07/16/00/2019-acc-aha-guideline-on-primary-prevention-gl-prevention - American Heart Association’s 2021 Scientific Statement on Management of Stage 1 Hypertension in Adults With a Low 10-Year Risk for Cardiovascular Disease: Filling a Guidance Gap
https://www.ahajournals.org/doi/full/10.1161/HYP.0000000000000195 - Centers for Disease Control and Prevention https://www.cdc.gov/bloodpressure/
- American Dental Association https://www.ada.org/resources/research/science-and-research-institute/oral-health-topics/hypertension
- Bowen DM (ed.) and Pieren JA (ed.). Darby and Walsh Dental Hygiene: Theory and Practice (5th edition). St. Louis: Elsevier; 2020.
- Little JW, Falace DA, Miller CS and Rhodus NL. Dental Management of the Medically Compromised Patient (9th edition). St. Louis: Elsevier; 2018.
- Malamed SF. Medical Emergencies in the Dental Office (7th edition). St. Louis: Mosby Elsevier; 2015.
- Pickett FA and Gurenlian JR. Preventing Medical Emergencies: Use of the Medical History in Dental Practice (3rd edition). Baltimore: Wolters Kluwer Health, 2015.
FOOTNOTES
1 Persons includes young persons and children
2 Routine measurement of blood pressure by dental hygienists in young children in the oral care setting may not always be practical. Where it is feasible and appropriate to measure blood pressure (as in older children and adolescents, particularly in those with risk factors), tables and/or calculators can guide screening for hypertension (i.e., BP beyond the 95th percentile for sex, age, and height).
3 For decision making about initiation of procedures in children and adolescents, refer to “Hypertension in Children and Adolescents Fact Sheet.”
4 SBP = systolic blood pressure
5 DBP = diastolic blood pressure