
CDHO Advisory: Oral Cancer
COLLEGE OF DENTAL HYGIENISTS OF ONTARIO ADVISORY
ADVISORY TITLE
Use of the dental hygiene interventions of scaling of teeth and root planing including curetting surrounding tissue, orthodontic and restorative practices, and other invasive interventions for persons1 with oral cancer.
ADVISORY STATUS
Cite as College of Dental Hygienists of Ontario, CDHO Advisory Oral Cancer 2024-04-05
INTERVENTIONS AND PRACTICES CONSIDERED
Scaling of teeth and root planing including curetting surrounding tissue, orthodontic and restorative practices, and other invasive interventions (“the Procedures”).
SCOPE
DISEASE/CONDITION(S)/PROCEDURE(S)
Oral cancer
INTENDED USERS
Advanced practice nurses
Dental assistants
Dental hygienists
Dentists
Denturists
Dieticians
Health professional students
Nurses
Patients/clients
Pharmacists
Physicians
Public health departments
Regulatory bodies
ADVISORY OBJECTIVE(S)
To guide dental hygienists at the point of care relative to the use of the Procedures for persons who have oral cancer, chiefly as follows.
- Understanding the medical condition.
- Sourcing medications information.
- Taking the medical and medications history.
- Identifying and contacting the most appropriate healthcare provider(s) for medical advice.
- Understanding and taking appropriate precautions prior to and during the Procedures proposed.
- Deciding when and when not to proceed with the Procedures proposed.
- Dealing with adverse events arising during the Procedures.
- Record keeping.
- Advising the patient/client.
TARGET POPULATION
Adolescent (13 to 18 years)
Adult (19 to 44 years)
Middle Age (45 to 64 years)
Aged (65 to 79 years)
Aged 80 and over
Male
Female
Parents, guardians, and family caregivers of children, young persons and adults with oral cancer.
MAJOR OUTCOMES CONSIDERED
For persons who have oral cancer: to maximize health benefits and minimize adverse effects by promoting the performance of the Procedures at the right time with the appropriate precautions, and by discouraging the performance of the Procedures at the wrong time or in the absence of appropriate precautions.
RECOMMENDATIONS
UNDERSTANDING THE MEDICAL CONDITION
Terminology used in this Advisory
Resources consulted
- American Academy of Dermatology: Lichen Planus
- American Cancer Society: Detailed Guide: Oral Cavity and Oropharyngeal Cancer
- Medscape: Aphthous Stomatitis
- Medscape: Oral Leukoplakia
- Medscape: Oral Submucous Fibrosis
- Medscape: Premalignant Conditions of the Oral Cavity
- Merck Manual: Oral Squamous Cell Carcinoma
- Merck Manual: Systemic Sclerosis
Oral cancer
- comprises the largest group of cancers of the head and neck
- is also referred to as
- oral carcinoma
- oral cavity cancer
- oropharyngeal cancer
- mouth cancer
- tongue cancer; images of the lesion
- throat cancer; images of the lesion
Other terminology
- Acquired immunodeficiency syndrome (AIDS), a severe immunological disorder that is caused by the human immunodeficiency virus (HIV).
- Adjunctive therapy, adjuvant therapy, treatment supplementary to the primary therapy, for example chemotherapy (CDHO Advisory) or radiation therapy (CDHO Advisory) given after cancer surgery.
- Aphthous stomatitis or canker sores
- are among the most common oral mucosal lesions; images of the lesions
- when recurrent are
- termed recurrent aphthous ulcers
- regarded as a disorder of unknown etiology that can cause clinically significant morbidity
- manifest as one or several discrete, shallow, painful ulcers visible on the unattached mucous membranes
- as individual smaller ulcers that typically last 7–10 days
- as larger ulcers, which may
- last weeks or months
- scar when healing.
- Candida, oral candidiasis, also termed thrush or oral moniliasis, is
- a yeast infection of the mouth or throat
- most commonly caused by Candida albicans.
- Chemotherapy (CDHO Advisory), use of medications to treat cancer.
- Dose-response relation, a complex statistical function that
- expresses the correlation between the amount of harmful chemical, beneficial medication, or another type of measurable cause delivered to the body or organ, and the effect as measured by the occurrence of a specific outcome
- when established with rigorous research provides strong but nonetheless insufficient evidence that the cause does in fact create the effect
- may not exist between some causes, such as viral infection, and some effects that are definitively linked with particular causes, such as a particular viral disease.
- Dysarthria, a condition that
- results in distorted, slurred or slow speech that can be difficult to understand
- is caused by problems in the muscles used in speaking arising from
- weakness of the muscles
- difficulty in controlling or coordinating the muscles
- differs from dysphasia.
- Dysgeusia, distortion of the sense of taste.
- Dysphagia, difficulty, discomfort or pain on swallowing.
- Dysphasia, a member of a group of speech disorders in which there is impairment of the power of expression by speech, writing, or signs, or impairment of the power of comprehension of spoken or written language; the more severe forms of dysphasia are called aphasia.
- Epstein-Barr virus (EBV)
- causes infectious mononucleosis, also called glandular fever, characterized by
- fever
- sore throat
- swollen lymph glands
- is a member of the herpesvirus family
- is one of the most common human viruses
- is transmitted by saliva
- occurs worldwide
- infects most persons at some time during their lives.
- causes infectious mononucleosis, also called glandular fever, characterized by
- Erythroplakia, erythroplasia, a reddened patch with a velvety surface that is
- found in the mouth
- in more than half of its instances a precursor to cancer
- the most common potentially malignant oral disorder, along with leukoplakia
- images of the lesion.
- Fibrosis, thickening and scarring of connective tissue, chiefly a consequence of inflammation or injury.
- Graft-versus-host disease, a complication that can occur after a bone marrow transplant in which the newly transplanted bone marrow attacks the transplant recipient’s body.
- Herpes simplex virus (HSV)
- causes
- cold sores around the mouth or face
- genital herpes, a sexually transmitted disease
- may spread
- even when sores are not present
- from mothers to their babies during childbirth.
- causes
- HIV/AIDS (CDHO Advisory) is a disease called acquired immunodeficiency syndrome (AIDS) caused by the human immunodeficiency virus (HIV), a virus which
- causes acquired immune deficiency syndrome
- progressively destroys the body’s immune system.
- Human papilloma virus (HPV)
- is one of the most common virus groups; of its 120 types, HPV-16 and HPV-18 are
- the prime high-risk factors for oral cancer
- believed to be the fastest-growing risk factor for oral cancer
- affects the skin and mucosal areas
- is spread by sexual contact especially at a young age.
- is one of the most common virus groups; of its 120 types, HPV-16 and HPV-18 are
- Immunosuppression (CDHO Advisory), the reduction of the body’s normal immune response to invasion by foreign substances; it may be
- intentional, as in reduction of the immune response to prevent rejection of a transplanted organ
- incidental, arising as a side effect of radiation therapy (CDHO Advisory) or chemotherapy (CDHO Advisory).
- Independent risk factor, an established risk factor that is unrelated to one or more other established risk factors.
- Indurated, induration, hardening of soft tissue.
- Labial commissure, of the mouth, junction of upper and lower lips at the angle of the mouth.
- Lesion, a term variously and loosely used in medicine to refer to such things as
- any abnormality of tissue in the body, including the mouth and skin
- any localized abnormal structural change in a bodily part
- a mass especially before a definite diagnosis is established
- cancer
- an injury to living tissue, such as a cut or break in the skin.
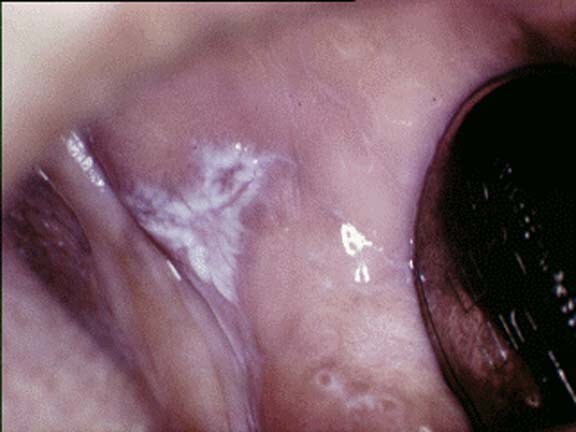
- Leukoplakia, a whitish patch that
- occurs in the mouth
- cannot be removed with a gauze swab
- is the most common potentially malignant oral disorder, along with erythroplakia
- when red-and-white speckled, is most likely to be potentially malignant when it
- is associated with the use of tobacco
- cannot be characterized clinically or pathologically as any other disease
- is not associated with any other physical or chemical causative agent
- images of the lesion
- Lichen planus, a common inflammatory disease of the skin and mouth which
- affects some 1–2 percent of the population
- may be an autoimmune disorder
- images of the lesion.
- Lichenoid mucosal reaction, condition resembling lichen planus that, with periodontal disease, occurs as part of graft-versus-host disease.
- Malignant, tending to metastasize; cancerous.
- Metastasis, when cancer cells break away from the primary tumor and spread to other organs through the blood stream or the lymphatic system.
- Mucositis, inflammation of the mucous membranes lining the entire digestive tract including the mouth.
- Myeloablation, a preparative treatment that eliminates the bone marrow’s ability to produce blood cells.
- Myelosuppression, suppression of bone marrow, which may be
- a serious side-effect of chemotherapy (CDHO Advisory)
- an intended effect of treatment for certain blood diseases.
- Occurrence, a term used in epidemiology to provide information about diseases and their trends, commonly measured by
- mortality, the number of deaths yearly per 1000 of population at risk
- incidence, the number of new cases yearly per 100,000 of population at risk
- prevalence, as defined for cancer, the number or percent of people alive on a certain date in a population who have been diagnosed with cancer.
- Oral submucous fibrosis, a chronic debilitating disease of the oral cavity that
- is characterized by inflammation and progressive fibrosis of the submucosal tissues
- is caused by betel quid chewing, practiced predominately in Southeast Asia and India, and which may also be found in some immigrant communities
- results in progressive rigidity eventually impairing the ability to open the mouth
- involves any part of the oral cavity
- may become cancerous.
- Oral ulcer, an open lesion, often painful, inside the mouth or upper throat, an alternative name for
- a mouth ulcer images of the lesion
- an aphthous ulcer images of the lesion
- aphthous stomatitis, also known as a canker sore
- a malignant ulcer.
- Osteoradionecrosis, bone necrosis that
- is secondary to radiation therapy (CDHO Advisory) and superimposed infection
- arises because radiation destroys normal cells and blood vessels, and not only tumour cells.
- Palliative care, services of care for persons towards the end of life with terminal illnesses such as cancer, when the focus of the care
- is relieving symptoms
- attending to physical and spiritual needs.
- Persistence, as used in connection with oral lesions that could be the beginnings of oral cancer
- is defined as a duration exceeding two to four weeks
- effectively labels the lesion as suspicious until proven otherwise.
- Primary therapy, initial treatment used to reduce a cancer, and followed by adjunctive therapy, such as chemotherapy (CDHO Advisory) and radiation therapy (CDHO Advisory).
- Retromolar pad, a cushion-like mass of tissue located on the alveolar process of the mandible behind the area of the last natural molar tooth.
- Radiation therapy (CDHO Advisory), radiotherapy, x-ray therapy, or irradiation, the use of ionizing radiation to kill cancer cells and shrink tumors.
- Risk factor, a term
- used strictly to identify anything that affects the person’s chances of developing a disease such as oral cancer
- used loosely to refer to things that in themselves may not affect the person’s chances of developing a disease such as oral cancer but which may signal the presence of things that are risk factors as strictly defined; for example, problematic dentition and poor oral hygiene may signal smoking and considerable alcohol consumption, which are independent risk factors for oral cancer
- that informs medical history-taking and examination, which takes account of evidence based on dose-response relations such that between the type and amount of smoking and the development of oral cancer
- that, in the absence of clear-cut epidemiological data, often cannot be quantified or even rank-ordered for importance.
- Sicca syndrome, a term reserved for the combination of dryness of the mouth and eyes, regardless of cause; when accompanied by lymphocyte infiltration of the salivary glands is named Sjögren syndrome (CDHO Advisory).
- Supportive care, services of care to help persons meet the physical, emotional and spiritual challenges arising from
- cancer
- treatment of the cancer.
- Systemic sclerosis, scleroderma, a rare chronic disease of unknown cause characterized by diffuse fibrosis, degenerative changes, and vascular abnormalities in the skin, joints, and internal organs.
- Squamous cell carcinoma, a type of cancer that occurs in the skin and the mouth.
- Trismus, restriction to the opening of the mouth caused by trauma, surgery, or radiation associated with the treatment of oral cancer.
- Xerostomia, abnormal dryness of the mouth resulting from decreased secretion of saliva; has various causes including
- chemotherapy (CDHO Advisory)
- head and neck radiation therapy (CDHO Advisory)
- sicca syndrome
- Sjögren syndrome (CDHO Advisory)
- some medications.
Overview of oral cancer
Resources consulted
- Canadian Cancer Society: Canadian Cancer Statistics
- Canadian Cancer Society: Oral Cancer
- Canadian Dental Association Oral Cancer: Just the Facts
- Canadian Dental Association: Oral Cancer
- Canadian Medical Association: Hematopoietic stem cell transplantation: a primer for the primary care physician
- Cancer.Net (American Society of Clinical Oncology): Oral and Oropharyngeal Cancer Statistics
- College of Dental Hygienists of Ontario: Chemotherapy Fact Sheet
- College of Dental Hygienists of Ontario: Gastrointestinal Tract Tumours Advisory
- College of Dental Hygienists of Ontario: Hematopoietic Cell Transplantation Fact Sheet
- College of Dental Hygienists of Ontario: Human Papillomavirus Fact Sheet
- College of Dental Hygienists of Ontario: Lichen Planus Fact Sheet
- College of Dental Hygienists of Ontario: Oral Cancer Fact Sheet
- College of Dental Hygienists of Ontario: Radiation Therapy Fact Sheet
- College of Dental Hygienists of Ontario: Sjögren Syndrome Fact Sheet
- Government of Canada: Oral Cancer
- Heads Up! — A Call for Dentists to Screen for Oral Cancer
- MedlinePlus: Oral Cancer
- Medscape: Cancers of the Oral Mucosa
- Medscape: Candidiasis, Mucosal
- Medscape: Leukoplakia, Oral
- Medscape: Oral Submucous Fibrosis
- Medscape: Premalignant Conditions of the Oral Cavity
- National Cancer Institute: Oral Complications of Chemotherapy and Head/Neck Radiation
Oral cancer
- Nature
- some 90 percent of instances of oral cancer are of the type squamous cell carcinoma
- is the sixth most common cancer in the world
- is a devastating disease with severe consequences to the
- individual
- society.
- Sites
- lower lip, which manifests at the mucocutaneous junction as
- a small, persistent lump
- an ulcer
- a scabbed lesion
- intraorally, including
- the most common site, the middle third of the lateral margin of the tongue, which in the later stages may manifest as
- a lesion growing on the surface of the tongue
- an ulcer
- an area of surface ulceration with induration
- the second most common site, the anterior floor of the mouth where it
- is often associated with leukoplakia
- is indurated
- ulcerates
- causes problems with speech
- common sites
- the posterior tongue/floor of the mouth
- the palate and tonsillar area (which may be classified as oropharyngeal cancer rather than oral cavity cancer)
- other sites, such as the
- alveolus or gingiva, in which the oral cancer
- usually appears as a lump or ulcer mostly in the
- mandibular premolar region
- molar region
- invades the underlying alveolar bone in 50 percent of cases
- may loosen adjacent teeth
- usually appears as a lump or ulcer mostly in the
- buccal mucosa, where it
- mostly occurs
- at the commissure
- or in the retromolar area
- manifests chiefly as ulcerated lumps
- may arise in leukoplakia
- mostly occurs
- alveolus or gingiva, in which the oral cancer
- the most common site, the middle third of the lateral margin of the tongue, which in the later stages may manifest as
- may occur simultaneously in more than one site in the mouth
- as an additional primary cancer
- in as many as 10–15 percent of persons with oral cancer.
- lower lip, which manifests at the mucocutaneous junction as
- Clinical characteristics
- by inspection
- are highly variable
- include
- ulcers: a typical malignant ulcer
- is hard
- has heaped-up and often everted or rolled edges
- has a granular floor
- red patches, erythroplakia, that
- prove to be malignant in more than half of instances
- are level with or depressed below the surrounding mucosa
- occur in women and men in their sixth and seventh decades
- typically involve one of these areas
- floor of the mouth
- anterior of the tongue
- soft palate
- white patches, leukoplakia, which, when persistent, may be
- oral cancer or a precursor to it
- lichen planus, which is not necessarily cancerous
- candidiasis, which is not cancerous
- lumps
- fissures
- ulcers: a typical malignant ulcer
- by palpation to detect
- lesions in the mouth that are
- indurated
- fixed to tissues
- cervical lymph nodes that are
- enlarged by metastases (oral cancer chiefly metastasizes first to the lymph nodes in the anterior neck)
- indurated
- fixed to tissues
- swollen salivary glands
- thickened cheeks.
- lesions in the mouth that are
- by inspection
- Symptoms and signs may include one or more of
- bleeding in the mouth
- dysgeusia
- dentures that no longer fit
- dysphagia
- loose teeth
- lump(s) in the
- gums
- lip
- mouth, including roof
- tongue
- tonsil area
- pain in the mouth that is persistent
- precancerous conditions on the lips or in the mouth
- erythroplakia
- leukoplakia
- dysarthria or similar difficulties with speaking
- swollen cervical lymph nodes
- swollen salivary glands
- thickening in the cheek
- ulcer in the mouth that does not heal.
- Risk factors
- oral conditions such as
- general neglect of oral health and problematic dentition signalled by
- missing teeth
- teeth with abrasive edges
- ill-fitting dentures
- oral lichen planus
- lupus erythematosus (CDHO Advisory) for which treatment involves immunosuppression (CDHO Advisory)
- general neglect of oral health and problematic dentition signalled by
- tobacco and alcohol use, which are independent risk factors for
- oral cavity cancer
- oropharyngeal cancer
- head and neck cancer
- heavy tobacco smokers, compared to non-smokers: 20-fold greater risk
- cigarette smokers, compared to non-smokers, for
- smokers of low/medium-tar cigarettes: 8.5-fold greater risk
- smokers of high-tar cigarettes: 16.4-fold greater risk
- heavy alcohol drinkers
- 5-fold greater risk
- who also smoke: 50-fold greater risk
- persons with the highest levels of smoking and alcohol consumption compared with persons who neither drink nor smoke, 80-fold greater risk
- betel-quid chewing and tobacco-chewing, which
- are important risk factors in persons from specific geographic areas, such as Southeast Asia
- may accompany immigration to North America and elsewhere
- lead to oral submucous fibrosis
- infective agents, which include
- viruses, such as
- human papillomavirus, HPV 16 and 18, which are particularly associated with oral cancers in
- lingual and palatine tonsils
- soft palate
- base of the tongue
- Epstein-Barr virus
- herpes simplex virus
- human immunodeficiency virus (CDHO Advisory)
- human papillomavirus, HPV 16 and 18, which are particularly associated with oral cancers in
- viruses, such as
- social instability or behaviours that lead to social instability are linked to increased risk of oral cancer, though other risk factors are likely to be involved, such as
- oral health
- diet
- prolonged, repeated exposure of the lips to the sun
- previous head and neck cancer
- immune-deficient states, which may predispose especially to lip cancer, such as occurs with
- immunosuppression (CDHO Advisory) for a solid-organ transplant
- diabetes (CDHO Advisory)
- systemic sclerosis
- occupational exposures to agents such as
- asbestos
- perchloroethylene
- radiation (CDHO Advisory)
- family history of head, neck or oral cancer
- diet low in fresh vegetables, such as beta-carotene-rich vegetables and citric fruits (CDHO Advisory)
- alcohol-based mouthwash, which is the subject of controversy because
- the effect of the alcohol in mouthwash appears to resemble that of alcohol used for drinking
- heavy smokers and drinkers may also be heavy users of mouthwash
- the contribution of mouthwash use to oral cancer risk is believed small.
- oral conditions such as
- Prognosis: the majority of oral cancers are still found at the late stage
- resulting in
- high death rate five years beyond the date of diagnosis
- high treatment-related morbidity in survivors
- arising from
- insufficient public awareness of
- oral cancer
- the risk factors of oral cancer
- insufficient screening by medical and oral health professionals for early oral cancer detection, which is
- the critical prognostic factor in cancer
- of high value as confirmed by the 5-year disease-free rate for
- early oral cancer: 70 percent
- advanced oral cancer: 30 percent or less.
- insufficient public awareness of
- resulting in
- Occurrence: oral cancer
- is uncommon before the age of 40
- shows
- the highest incidence in the 6th and 7th decades
- 2:1 male predominance
- is increasing in younger persons, a trend of growing concern
- is found worldwide, with the highest incidence in African and Asian countries
- in the form of lip cancer appears to be decreasing
- in Canada, estimates for 2020 (unless otherwise noted) indicate
- new cases
- all residents of Canada: 5,400
- men: 3,700
- women: 1,650
- lifetime probability of developing oral cancer
- men: 1.5% (2015 estimate)
- women: 0.7% (2015 estimate)
- deaths in Canada
- all residents of Canada: 1,500
- men: 1,050
- women: 440
- lifetime probability of dying from oral cancer
- men: 0.5% (2015 estimate)
- women: 0.3% (2015 estimate)
- the five-year survival rate as 64 percent (2012–2014 predicted net survival) compared to that for
- cervical cancer: 72 percent
- melanoma cancers: 88 percent
- prostate cancer: 93 percent
- new cases
- in the United States in 2023, estimates indicate that
- some 54,540 persons will be newly diagnosed (with oral cavity or oropharyngeal cancer)
- the rate of occurrence is increasing
- occurrence is generally higher in ethnic minorities, as in other developed countries
- males are affected more than twice as frequently than females
- oral cancer predominates in middle-aged and older persons.
- Spread, within the body
- is local, involving destruction of adjacent tissue especially muscle and bone
- is by metastasis, which is
- initially to the anterior cervical lymph nodes
- later to the liver and skeleton.
- Medical investigation involves
- biopsy of the suspected area
- imaging tests such as
- X-ray
- ultrasound
- CT scan
- MRI
- general investigations, especially in the later stages for
- anemia (CDHO Advisory)
- liver function (CDHO Advisory).
- Treatment
- surgery, often the treatment of choice
- chemotherapy (CDHO Advisory)
- radiation therapy (CDHO Advisory).
- Prevention of oral cancer and its consequences
- early detection
- reduction of risk factors.
Multimedia and images
- Aphthous ulcers and cold sores
- Aphthous Ulcers (Medscape)
- Cold Sore (MedlinePlus)
- Erythroplakia
- Cancer, oral general
- Oral cancers and non-cancerous conditions (Oral Cancer Foundation)
- Cancer, oral mucosa
- Cancers of the Oral Mucosa (Medscape)
- Cancer, tongue
- Oral Cancer (Canadian Dental Association)
- Cancer, lip
- Lip Cancer Picture (Hardin MD Super Site Sample)
- Leukoplakia
- Oral Leukoplakia (Medscape)
- Mouth ulcer
- Mouth ulcer (AbsoluteAstronomy.com)
- Oral conditions, various
- Oral photographs (entusa.com)
- Oral lichen planus
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comorbidity, complications and associated conditions
Comorbid conditions are those which co-exist with oral cancer but which are not believed to be caused by it. Complications and associated conditions are those that may have some link with it. Distinguishing among comorbid conditions, complications and associated conditions may be difficult in clinical practice.
For oral cancer, comorbid conditions, acute and chronic complications and conditions occur with the cancer alone or with the cancer and its treatment especially with chemotherapy (CDHO Advisory) and radiation therapy (CDHO Advisory); these
- commonly include
- infection, such as Candidiasis
- mucositis
- pain
- salivary gland dysfunction
- may lead to secondary complications such as
- dehydration
- dysgeusia
- malnutrition
- xerostomia
- may cause the mouth to be a source of systemic infection in myelosuppressed cancer patients
- may through radiation of the head and neck
- irreversibly injure
- bone
- muscle
- oral mucosa
- vasculature
- result in severe consequence, such as
- osteonecrosis (CDHO Advisory)
- osteoradionecrosis
- rampant dental caries
- soft tissue necrosis
- trismus
- irreversibly injure
- vary by cancer therapy: estimates of frequencies of comorbidities, complications and associated conditions include
- adjunctive chemotherapy: 10 percent
- primary chemotherapy: 40 percent
- graft-versus-host disease which
- occurs in 80 percent of unrelated-donor transplant recipients
- arises from hematopoietic stem cell transplantation involving myeloablative conditioning regimens
- may include
- sicca syndrome
- periodontal disease
- lichenoid mucosal reaction of the mouth
- head and neck radiation therapy (CDHO Advisory) to fields involving the oral cavity: 100 percent
- can compromise delivery of optimal cancer therapy and even undermine survival, through
- dose reduction or treatment-schedule modifications needed to allow healing of oral lesions
- discontinuation of cancer therapy in cases of severe oral effects which the patient may no longer be able to tolerate
- result from processes that originate
- in the cancer and its consequences, including
- spread
- associated symptoms and signs
- in the particular side effects of chemotherapy (CDHO Advisory) and radiation therapy (CDHO Advisory)for which the oral cavity is at high risk, which include
- stopping the growth of rapidly dividing cells, in particular
- the cancer cells, as intended
- the normal cells in the lining of the mouth, which also divide rapidly, so that the treatment may prevent cells in the mouth from reproducing, an important process of normal repair
- upsetting the healthy balance of oral bacteria though changes that
- occur in
- the lining of the mouth
- the production of saliva
- render the mouth prone to sores, infections and tooth decay
- promote inflammation of the mucous membrane in the mouth
- facilitate infections in the mouth that travel through the bloodstream, reaching and affecting tissues and organs
- occur in
- increasing the susceptibility to wear and tear that occurs from normal use of the mouth, teeth, and jaws
- creating tooth decay and gum disease
- stopping the growth of rapidly dividing cells, in particular
- in the surgical treatment for the cancer, including post-surgical
- disfigurement of the face, head, and neck
- dysarthria
- dysgeusia.
- in the cancer and its consequences, including
Oral health considerations
Dental hygiene has an important role
- In the early detection of oral cancer because
- currently, too many oral cancers remain undetected until they have reached an advanced stage
- early detection and treatment
- substantially improves survival rates
- is an important goal in preventive healthcare
- persistent oral-area ulcers, lumps, red patches, or white patches should be regarded as suspicious until medical investigation proves them otherwise
- screening is a 3-part, routine procedure for all patients/clients that
- is within the scope of practice of dental hygienists
- comprises
- review of the medical and health history, which should include
- questions about risk factors
- providing appropriate advice
- inspection and palpation of the
- cervical lymph nodes
- salivary glands
- lips and cheeks
- intraoral examination, which explicitly includes the
- buccal and labial mucosa
- mandibular buccal and lingual gingiva
- retromolar pad
- maxillary buccal and palatal gingiva
- hard and soft palate, tonsillar tissues and uvula
- floor of mouth
- tongue surfaces
- dorsal
- lateral
- ventral
- review of the medical and health history, which should include
- carefully records the location, colour and texture of suspicious lesions, preferably on a standard topographic diagram.
- In managing the oral complications of cancer therapy, which includes
- prior to cancer therapy, assessment of oral status to find and treat oral problems to prevent or lessen the severity of oral complications, such as
- periodontal disease
- advanced caries
- periapical lesions
- identification of high-risk populations
- patient/client education
- initiation of pretreatment interventions
- timely management of lesions.
- prior to cancer therapy, assessment of oral status to find and treat oral problems to prevent or lessen the severity of oral complications, such as
- In promptly referring any suspicious lesion to the family physician or an appropriate specialist.
- In reducing infection risk by attention to oral hygiene prior to treatments for oral cancer.
- In providing care to persons insufficiently connected with the oral healthcare system.
- In instructing patients/clients in oral self-inspection and the importance of reporting changes in the mouth to the appropriate healthcare provider.
- In continuing to provide oral healthcare to persons with advanced oral cancer.
MEDICATIONS SUMMARY
Sourcing medications information
- Adverse effect database
- Health Canada’s Marketed Health Products Directorate (MedEffect Canada) toll-free 1-866-234-2345
- Health Canada’s Drug Product Database
- Specialized organizations
- Medications considerations
All medications have potential side effects whether taken alone or in combination with other prescription medications, or as over-the-counter (OTC) or herbal medications. - Information on herbals and supplements
Types of medications
Chemotherapy (CDHO Advisory), which
- is combined with other treatments as part of a treatment plan particularized for the individual patient
- commonly involves
- 5-fluorouracil (5-FU, Adrucil®)
- bleomycin
- carboplatin (Paraplatin®)
- cisplatin (Platinol®-AQ)
- methotrexate (Rheumatrex®, Trexall®)
- also includes
- docetaxel injection (Taxotere®)
- paclitaxel injection (Abraxane®, Taxol®)
- may require a rescue agent to counteract the damaging effects of some chemotherapy medications, such an agent is
- amifostine injection (Ethyol®)
Side effects of medications
See the links above to the specific medications.
THE MEDICAL AND MEDICATIONS HISTORY
The medical and medications history-taking should
- Focus on screening the patient/client prior to treatment decision relative to
- key symptoms and their duration
- medications considerations
- contraindications
- complications
- comorbidities
- associated conditions.
- Explore the need for advice from the appropriate primary or specialized care provider(s).
- Inquire about
- the persistence of lesions potentially indicative of undetected oral cancer, with particular reference to
- the length of time the patient/client has been aware of the lesion
- whether the lesion has been adequately investigated
- the patient/client’s understanding and acceptance of the need for oral healthcare
- medications considerations, including over-the-counter medications, herbals and supplements
- problems with previous dental/dental hygiene care
- problems with infections generally and specifically associated with dental/dental hygiene care
- the patient/client’s current state of health
- how the patient/client’s current symptoms relate to
- oral health
- health generally
- recent changes in the patient/client’s condition.
- the persistence of lesions potentially indicative of undetected oral cancer, with particular reference to
IDENTIFYING AND CONTACTING THE MOST APPROPRIATE HEALTHCARE PROVIDER(S) FOR ADVICE
Identifying and contacting the most appropriate healthcare provider(s) from whom to obtain medical or other advice pertinent to a particular patient/client
- Record the name of the physician/primary care provider most closely associated with the patient/client’s healthcare, and the telephone number.
- Obtain from the patient/client or parent/guardian written, informed consent to contact the identified physician/primary healthcare provider.
- Use a consent/medical consultation form, and be prepared to securely send the form to the provider.
- Include on the form a standardized statement of the Procedures proposed, with a request for advice on proceeding or not at the particular time, and any precautions to be observed.
UNDERSTANDING AND TAKING APPROPRIATE PRECAUTIONS
Infection Control
Dental hygienists are required to keep their practices current with infection control policies and procedures, especially in relation to
- the CDHO’s Infection Prevention and Control Guidelines (2024)
- relevant occupational health and safety legislative requirements
- relevant public health legislative requirements
- best practices or other protocols specific to the medical condition of the patient/client.
DECIDING WHEN AND WHEN NOT TO INITIATE THE PROCEDURES PROPOSED
The dental hygienist
- on discovery of a suspicious lesion should
- promptly refer the patient/client to the primary care physician or the appropriate specialist
- implement the Procedures cautiously or even avoid the area altogether to prevent trauma to or alteration of the lesion prior to the dental hygienist’s obtaining medical advice.
- in the interest of coordinating care, minimizing adverse effects or avoiding delay in cancer treatment, and out of consideration for the patient/client, the dental hygienist should not implement the Procedures prior to receiving advice from the primary care physician or appropriate specialist if the oral-cancer patient/client
- is scheduled for major oral surgery for oral cancer
- is about to undergo or is undergoing chemotherapy (CDHO Advisory)
- is about to undergo or is undergoing radiation therapy (CDHO Advisory)
- has been advised about the need for such advice by a physician or specialist.
- with an otherwise healthy patient/client whose cancer treatment is proceeding normally the dental hygienist should implement the Procedures, though these may be postponed pending medical advice,
- if the patient/client has symptoms or signs suggestive of comorbidity, complication or associated condition
- not recently or ever sought and received such advice relative to oral healthcare procedures
- recently changed cancer-related or other significant medications, under medical advice or otherwise
- recently experienced changes in his/her medical condition such as medication or other side effects of cancer treatment
- is deeply concerned about any aspect of his or her medical condition.
DEALING WITH ANY ADVERSE EVENTS ARISING DURING THE PROCEDURES
Dental hygienists are required to initiate emergency protocols as required by the College of Dental Hygienists of Ontario’s Standards of Practice, and as appropriate for the condition of the patient/client.
First-aid provisions and responses as required for current certification in first aid.
RECORD KEEPING
Subject to Ontario Regulation 9/08 Part III.1, Records, in particular S 12.1 (1) and (2), for a patient/client with a history of oral cancer, the dental hygienist should specifically record
- A summary of the medical and medications history.
- Any advice received from the physician/primary care provider relative to the patient/client’s condition.
- The decision made by the dental hygienist, with reasons.
- Compliance with the precautions required.
- All Procedure(s) used.
- Any advice given to the patient/client.
ADVISING THE PATIENT/CLIENT
The patient/client is urged to alert any healthcare professional who proposes any intervention or test that he or she has a history of oral cancer.
As appropriate, discuss
- The importance of the patient/client’s
- self-checking the mouth regularly for suspicious signs or symptoms
- reporting any changes in the mouth to the appropriate healthcare provider.
- The need for regular oral health examinations and preventive oral healthcare.
- Oral self-care including information about
- choice of toothpaste
- tooth-brushing techniques and related devices
- dental flossing
- mouth rinses
- management of a dry mouth.
- The importance of an appropriate diet in the maintenance of oral health.
- For persons at an advanced stage of oral cancer
- regimens for oral hygiene as a component of supportive care and palliative care
- the role of the family caregiver, with emphasis on maintaining an infection-free environment through hand-washing and, if appropriate, wearing gloves.
- Medication side effects such as dry mouth, and recommend treatment.
- Scheduling and duration of appointments for patients/clients who are debilitated.
- Comfort level while reclining, and stress and anxiety related to the Procedures.
- Mouth ulcers and other conditions of the mouth relating to oral cancer, comorbidities, medications or diet.
- Pain management.
BENEFITS/HARMS OF IMPLEMENTING THE RECOMMENDATIONS
POTENTIAL BENEFITS
- Promotion of health through oral health and oral hygiene for persons who have oral cancer.
- Earlier detection of oral cancer by
- encouraging routine oral cancer screening by dental hygienists for all patients/clients
- promoting
- awareness among dental hygienists of oral cancer risk and risk factors
- self-checking by patients/clients.
- Integration of dental hygiene with healthcare for persons at all stages of oral cancer.
- Reducing the risk that oral health needs are unmet.
POTENTIAL HARMS
- Causing diagnosis to be delayed by failure to recognize the significance of suspicious lesions or symptoms.
- Performing the Procedures at an inappropriate time, such as
- when the patient/client’s is receiving or about to receive treatment for which prior medical advice is required
- in the presence of comorbidities, complications or associated conditions for which prior medical advice is required
- in the presence of acute oral infection without prior medical advice.
- Disturbing the normal dietary and medications routine of a person with oral cancer.
- Inappropriate management of pain or medication.
CONTRAINDICATIONS
CONTRAINDICATIONS IN REGULATIONS
Identified in the Dental Hygiene Act, 1991 – O. Reg. 218/94 Part III
ORIGINALLY DEVELOPED
2010-07-15
DATE OF LAST REVIEW
2010-07-15; 2020-01-31; 2024-04-05
ADVISORY DEVELOPER(S)
College of Dental Hygienists of Ontario, regulatory body
Greyhead Associates, medical information service specialists
SOURCE(S) OF FUNDING
College of Dental Hygienists of Ontario
ADVISORY COMITTEE
College of Dental Hygienists of Ontario, Practice Advisors
COMPOSITION OF GROUP THAT AUTHORED THE ADVISORY
Dr Gordon Atherley
O StJ , MB ChB, DIH, MD, MFCM (Royal College of Physicians, UK), FFOM (Royal College of Physicians, UK), FACOM (American College of Occupational Medicine), LLD (hc), FRSA
Dr Kevin Glasgow
MD, MHSc, MBA, DTM&H, CHE, CCFP, DABPM, LFACHE, FCFP, FACPM, FRCPC
Lisa Taylor
RDH, BA, MEd
Janet Aquilina-Arnold
RDH
Kyle Fraser
RDH, BComm, BEd, MEd
Carolle Lepage
RDH, BEd
ACKNOWLEDGEMENTS
The College of Dental Hygienists of Ontario gratefully acknowledges the Template of Guideline Attributes, on which this advisory is modelled, of The National Guideline Clearinghouse™ (NGC), sponsored by the Agency for Healthcare Research and Quality (AHRQ), U.S. Department of Health and Human Services.
Denise Lalande
Final layout and proofreading
COPYRIGHT STATEMENT(S)
© 2010, 2020, 2024 College of Dental Hygienists of Ontario
FOOTNOTES
1 Persons includes young persons and children.